Blood Chemistry in the Physician Office Laboratory
April 11, 2024
Learning Objective: Examine blood chemistry in the physician office laboratory.
CLIA-waived chemistry tests using whole blood from capillary punctures have become popular in ambulatory practices. With the increase in diabetes and cardiovascular disease in the United States, patients with either (or both) of these metabolic diseases benefit from early diagnosis. Treatment is based on continued monitoring of glucose and hemoglobin A1c for diabetes and of cholesterol, lipid panels, and liver enzymes for cardiovascular diseases related to fatty deposits in the arteries.
Blood Glucose Testing
Learning Objective: Describe blood glucose testing.
Glucose is used as a fuel by all body cells. Under normal circumstances, it is the only substance used to nourish brain cells. Maintenance of blood glucose levels within a normal range is vital to homeostasis of the human body. Understanding the importance of glucose can help the medical assistant understand why glucose is the most frequently tested chemical analyte in the blood.
Elevated blood glucose levels are most often associated with diabetes mellitus. They also may indicate pancreatitis, endocrine disorders, or chronic renal failure. Diabetes mellitus is a disorder of carbohydrate metabolism that results in elevated blood and urine glucose levels. In diabetes mellitus, either the pancreas is unable to produce sufficient insulin to meet the body’s needs, or insulin resistance develops at the cellular level (see Chapter 24).
For the initial screening of a patient for diabetes type 2, a fasting blood sample is usually taken in the morning, after a fast of 10 to 12 hours. The patient’s fasting blood glucose (FBG) level should be less than 100 mg/dL. If it is higher than 105 mg/dL, the provider may request a blood glucose tolerance test (GTT). For this test, the fasting patient receives a sugary liquid to drink that contains 100 g of glucose. (The amount may be adjusted according to the patient’s weight.) A blood glucose level of less than 140 mg/dL after 2 hours is normal. A reading of more than 200 mg/dL after 2 hours may indicate diabetes. A reading between 140 and 199 mg/dL indicates impaired glucose tolerance or prediabetes.
Home Glucose Monitoring
Many CLIA-waived glucometers are available for professional and at-home use. The process the medical assistant uses in the ambulatory care facility for testing blood glucose is very similar to what the patient does at home (Procedure 34.6).
Home glucose monitoring is part of the treatment plan for diabetes mellitus (DM) management. Patients with type 1 DM or type 2 DM may need to test their blood glucose several times a day. Glucose levels may also be monitored by women with gestational diabetes, a condition seen during pregnancy in which the effect of insulin is partially blocked by hormones produced by the placenta (FIGURE 34.12).
The medical assistant may need to coach patients on how to test their blood glucose. If the patient’s glucose monitor is available, it is helpful to demonstrate the procedure using the monitor the patient will use. The patient should also do a return demonstration so the medical assistant can ensure that the patient is performing the procedure accurately.
When coaching a patient on using the glucose monitor, the medical assistant should discuss the following topics:
• Equipment and supplies required, and how to dispose of sharps
• How to calibrate the monitor when using new container of test strips
• How to perform a capillary puncture, which includes finding and cleaning the site, lancets to use, disposal of lancets, and how to apply the blood to the test strip
• How to run the test, read the result, and how to document the results (if needed by the provider). Some monitors allow patients to upload their test results using the patient portal; thus the provider can see the results between visits.
Hemoglobin A1c Testing
Learning Objective: Describe hemoglobin A1c testing.
Several methods can be used to measure the hemoglobin A1c level, including CLIA-waived handheld devices. Hemoglobin A1c is also described as glycosylated hemoglobin (sugar-coated hemoglobin). Glycosylated hemoglobin is the result of glucose irreversibly binding to the hemoglobin molecules in the RBCs. It is also referred to as the A1c.

FIGURE 34.12 Glucometer and supplies.
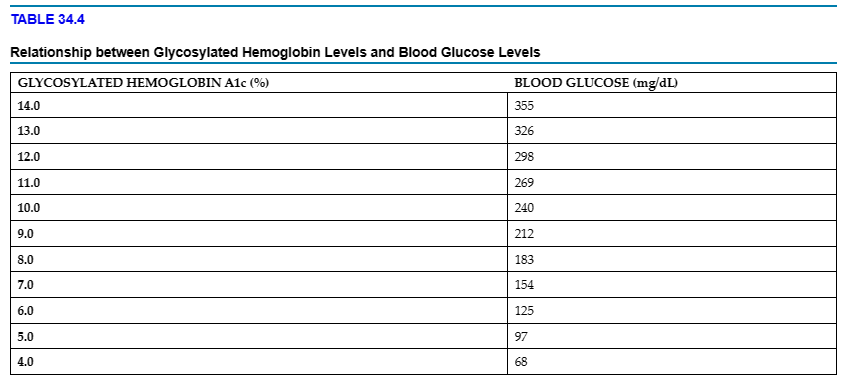
RBCs have a life span of approximately 120 days. Measuring the amount of glucose that has been irreversibly bound to hemoglobin provides an assessment of the average blood glucose during the 60 to 90 days before the test. The A1c test is performed every 3 months in patients with diabetes to monitor the person’s average blood glucose level during those months. An A1c value higher than normal indicates that the average blood glucose has been elevated during the past 2 to 3 months. A normal A1c level for a person without diabetes ranges from 4% to 5.6%. For patients with diabetes, the goal is to maintain the glycosylated hemoglobin level below 7%. In TABLE 34.4, glycosylated hemoglobin A1c levels are associated with blood glucose levels. With higher levels, the risk of developing complications from diabetes increases.
Home A1c Monitoring
Home A1c monitoring does not replace home blood glucose monitoring. Home A1c monitoring is another tool for the management of DM. Patients can perform A1c testing at home using instruments approved by the US Food and Drug Administration (FDA), such as the A1CNow SelfCheck (Bayer) and the in2it (II) Self-Test A1c System (Bio-Rad). The medical assistant may need to coach the patient on home A1c monitoring. The same topics addressed in the Home Glucose Monitoring section would apply to home A1c monitoring.
Cholesterol Testing
Learning Objective: Describe cholesterol testing.
Cholesterol is a fatlike substance (lipid) present in cell membranes. It is needed to form bile acids, steroid hormones, the coverings of our nerves, and some of our brain tissue. Cholesterol travels in the blood as distinct particles containing both lipids and proteins. These particles are called lipoproteins. The cholesterol level in the blood is determined partly by inheritance and partly by acquired factors, such as diet, calorie and nutrient balance, and level of physical activity.
Patients often are confused by cholesterol testing. Cholesterol is often a catchall term for both the cholesterol a person eats and the cholesterol that is produced in the body. A high blood level of low-density lipoprotein (LDL) cholesterol reflects an increased risk of heart disease. LDL cholesterol is often referred to as “bad” or “lousy” cholesterol. Lower levels of LDL cholesterol reflect a lower risk of heart disease. When too much LDL cholesterol circulates in the blood, it can slowly build up in the walls of arteries that feed the heart and brain. Together with other substances, it can form plaque, a thick and sticky deposit that can clog arteries. This condition is known as atherosclerosis. If a blood clot (thrombus) forms at the site of plaque, blood flow can be blocked in the coronary arteries of the heart muscle, causing a heart attack. If a clot blocks blood flow to part of the brain, a stroke may result. LDL results are often interpreted as follows:
LDL >100 mg/dL = Optimal
LDL 100–129 = Near or above optimal
LDL 130–159 = Borderline high
LDL 160–189 = High
LDL 190+ = Very high
About one-third to one-fourth of blood cholesterol is carried by high-density lipoprotein (HDL). HDL cholesterol is known as “good” or “healthy” cholesterol. High levels of HDL cholesterol seem to protect against heart attack. HDL can carry cholesterol away from the arteries and back to the liver. It is believed that cholesterol is removed from the lining of the arteries when high levels of HDL exist. Low levels of HDL cholesterol (i.e., lower than 40 mg/dL) may result in a greater risk of heart disease.
Adults older than 20 years of age should have a cholesterol test at least once every 5 years. Total cholesterol and the combination of LDL and HDL typically are screened and monitored. All three tests are considered screening tests, and elevated results require additional testing. In general, total cholesterol levels under 200 mg/dL are considered normal. Results over 240 mg/dL are considered elevated and may place a person in the high-risk category for coronary heart disease. An HDL cholesterol level of 40 mg/dL or higher is considered acceptable for men, and values of 50 or higher are acceptable for women. HDL levels below 40 mg/dL for men and below 50 mg/dL for women place a person at risk of coronary heart disease.
Although total cholesterol and HDL cholesterol levels are not significantly affected by food consumption, most providers prefer that patients fast from food and liquids, with the exception of water, for 12 hours before cholesterol levels are checked. If the total cholesterol is elevated, the provider is likely to order a lipid profile, which is a series of tests that measures the total cholesterol, HDL and LDL cholesterol levels, and triglyceride levels. Triglycerides are fat in the blood related to caloric intake. Therefore, the patient must be instructed to fast from all food and alcoholic beverages 12 hours before the triglyceride test or lipid profiles. Consistently high triglyceride levels may lead to heart disease, especially in people with low levels of “good” HDL cholesterol and high levels of “bad” LDL cholesterol and in people with diabetes type 2. Elevated levels of triglycerides are typically stored in belly fat and are associated with central obesity.
CLIA-waived cholesterol monitors can measure total cholesterol from a fingerstick specimen. The Cholestech LDX analyzer performs a lipid panel and provides a risk assessment using a capillary blood sample (Procedure 34.7). This system uses a cassette testing device capable of measuring glucose, total cholesterol (TC), HDL, LDL, very-low-density lipoprotein (VLDL), triglycerides, and the TC/HDL ratio. It uses a combination of testing methods to detect the color changes caused by each of the lipid panel analytes.
34.6 Critical Thinking Application
One of Anita’s favorite patients is in today, Sophie McCoy. She is 86 years young, still lives in her own home, and works in her garden every chance she gets. Sophie had a cholesterol screen at a local senior citizens health fair recently, and her results were as follows:
Total cholesterol 202 mg/dL, LDL 104 mg/dL, HDL 42 mg/dL
Given Sophie’s age and general good health, are the cholesterol results concerning? Are they normal, high, or low?
Thyroid Hormone Testing
Learning Objective: Describe thyroid hormone testing.
The thyroid gland is located anterior to the trachea in the throat. It produces the hormones triiodothyronine (T3) and thyroxine (T4). These hormones are essential for life and regulate body metabolism, growth, and development. The thyroid gland is influenced by hormones produced by two other glands found in the brain, the pituitary gland and the hypothalamus. The pituitary gland produces thyroid-stimulating hormone (TSH), and the hypothalamus produces thyrotropin-releasing hormone (TRH). (Regulation of thyroid hormone production and thyroid disorders are discussed in Chapter 24.)
CLIA-waived rapid diagnostic tests are available to qualitatively measure TSH. These tests are available for point-of-care testing (POCT). Using whole blood from a fingerstick, CLIA-waived tests can screen patients for hypothyroidism, which is deficient activity of the thyroid gland. Hypothyroidism is indicated with elevated TSH levels. The tests use lateral flow immunoassay technology housed in a plastic cassette. One such commercially available test is the ThyroTest Whole Blood TSH Test.
Reference Laboratory Chemistry Panels and Single Analyte Testing and Monitoring
Automated blood chemistry analyzers are often used to perform blood chemistry testing in a reference laboratory. It is common for several analytes to be detected at once. A provider may order a chemistry panel, such as a renal or liver panel, to determine the levels of several related analytes (FIGURE 34.13). Analytes commonly detected in the chemistry department are listed in TABLE 34.5. In general, serum from a clotted specimen is needed to perform these tests. Typical panels are shown in TABLE 34.6. As noted previously, laboratory reports, both electronic and paper, must provide their own reference ranges, along with each patient’s results. Different methodologies may generate different reference ranges and may use different units of measurement.