Arthritic Joint Diseases and Disorders
April 11, 2024
Arthritic Joint Diseases and Disorders
Learning Objective: Examine arthritic joint diseases and disorders, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Arthritis is a term that refers to any inflammatory joint condition. More than 54 million Americans have some form of arthritis. Arthritis is the leading cause of work disabilities in the United States. About 50% of arthritic cases are in those 65 years or older, though arthritis can occur at any age.
Arthritis can be caused by autoimmunity, infection, injury, and genetic conditions. The following sections discuss common arthritic conditions.
Osteoarthritis
Learning Objective: Discuss osteoarthritis, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Osteoarthritis (OA), also called degenerative joint disease (DJD), is the most common form of arthritis. OA can occur in any joint but most often affects the hands, hips, spine, and knees.
Osteoarthritis occurs when the cartilage at the end of the bones wears down, causing the bones to rub together, leading to permanent damage to the joint. Risk factors include genetics, being female, obesity, age, and injury to the joint. The signs and symptoms develop gradually and worsen over time. OA can cause pain, tenderness, stiffness, and swelling in joints, reducing the range of motion (FIGURE 20.14A). Bone spurs may form around the affected joint.
The provider will examine the affected joints and check the range of motion. X-rays, MRI, joint fluid analysis, and blood tests may be ordered to check for joint damage and rule out other types of arthritis. Treatment is focused on slowing the progression by maintaining a healthy weight, and limiting pain with the use of analgesics, NSAIDs, and duloxetine (Cymbalta). Additional interventions include physical therapy, occupational therapy, and cortisone injections in the joint to relieve pain. Joint replacement surgery (arthroplasty), such as a total hip or knee replacement, may also be done. The prognosis is good with surgery.

FIGURE 20.14 Types of arthritis. (A) Osteoarthritis. Note the presence of nodes in the proximal interphalangeal joints (Bouchard nodes) and distal interphalangeal joints (Heberden nodes). (B) Rheumatoid arthritis. Note the marked ulnar (elbow-like) deviation of the wrists. (C) Gouty arthritis. Note the tophi (stones) containing sodium urate crystals. From Swartz MH: Textbook of physical diagnosis, ed 6, Philadelphia, 2010, Saunders.
20.8
Critical Thinking Application
An 80-year-old male patient with arthritis comes into the office complaining of severe pain in his knees, hips, and lower back. The pain makes it impossible for him to get up onto the examination table. What should Suzanne do? Is this patient required to get onto the examination table? Why or why not?
Rheumatoid Arthritis
Learning Objective: Discuss rheumatoid arthritis, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Rheumatoid arthritis (RA) is an autoimmune and inflammatory disease. RA often starts in middle age and is common in older adults. A person can have the disease for a short time, or episodes may come and go. The severe form of RA is chronic.
With this autoimmune disease, the immune system attacks the healthy cells, causing inflammation in the joints, eyes, lungs, and mouth. Usually, it affects the wrist, finger, and knee joints. The lining of the joints becomes inflamed, causing damage to the joint tissue. Older adults and females are at most risk for RA, though women who have breastfed have a decreased risk. Other risk factors include genetics, cigarette use, and obesity. Signs and symptoms of RA include pain, achiness, stiffness, swelling, and tenderness in more than one joint (FIGURE 20.14B). Weight loss, fever, weakness, and fatigue can occur. Early stages of RA can be difficult to diagnose because the symptoms are similar to those of other joint diseases.
During the examination, the provider will check the reflexes, muscle strength, and the joints for signs of inflammation (e.g., swelling, redness, and warmth). Imaging tests (x-rays, MRI, and ultrasound [US]) may be done, along with blood tests, including the erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), rheumatoid factor (RF), and anti–cyclin citrullinated peptide (anti-CCP) antibodies. There is no cure for RA, but recent research has shown that early use of disease-modifying antirheumatic drugs (DMARDs) can increase the chances of remission.
Gout
Learning Objective: Discuss gout, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Gout (also called gouty arthritis) is a common form of inflammatory arthritis (FIGURE 20.14C). Gout can be acute or chronic, and attacks can last longer as time progresses.
The etiology is a buildup of uric acid in the body (FIGURE 20.15). Uric acid results from the breakdown of purines in foods (e.g., liver, dried peas and beans, and anchovies). The risk factors for gout include being male, a family history of gout, obesity, drinking alcohol, and eating too many purine-rich foods. Certain medications (e.g., diuretics, aspirin, niacin, and levodopa) may also increase the risk of gout. The signs and symptoms of gout include swollen, red, warm, and stiff joints. The great (big) toe is the most common site for gout, though it can affect the heel, ankle, knee, elbow, wrist, and fingers (see FIGURE 20.14C).
To diagnose gout, the provider will do a physical examination and order an x-ray and lab tests. The provider may take a sample of fluid from the inflamed joint area to look for uric acid crystals. Pseudogout has a similar presentation, but it is caused by calcium phosphate.
Treatment includes the following:
• NSAIDs can reduce pain and swelling.
• Corticosteroids (e.g., prednisone) can reduce inflammation.
• Colchicine (Colcrys, Gloperba) should be taken within the first 12 hours of the attack.
Full recovery may take up to 14 days. For additional treatments or to prevent future attacks by reducing the uric acid level in the blood, the person may need to take allopurinol, febuxostat, probenecid, or pegloticase. Patients are also encouraged to control their weight, limit alcohol intake, and reduce their dietary intake of meats and fish rich in purines.
Juvenile Arthritis
Learning Objective: Discuss juvenile arthritis, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Juvenile arthritis (JA) is a generic phrase for autoimmune, inflammatory, or rheumatic conditions that affect children under 16 years of age. Juvenile idiopathic arthritis (JIA) is the most common form of JA. Other types of JA include these:
• Juvenile dermatomyositis (JDM): Causes weakness and a rash on the eyelids and knuckles
• Juvenile systemic lupus erythematosus: An autoimmune disease that affects the kidneys, blood, skin, and joints
• Juvenile scleroderma: Causes skin to tighten and harden
• Kawasaki disease: Causes rash, swollen lymph nodes, fever, inflammation of blood vessels, and heart damage
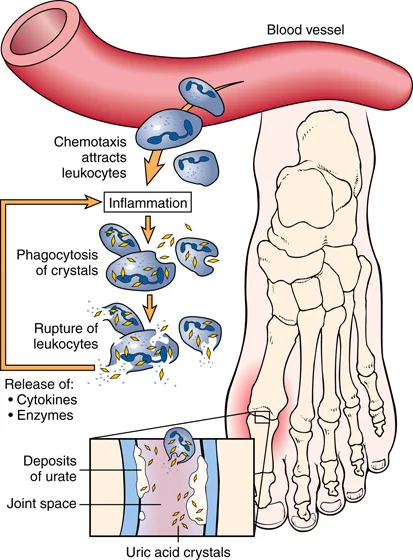
FIGURE 20.15 Gout is characterized by deposits of uric acid crystals in the connective tissue. The inflammation most often affects the joint of the big toe. From Damjanov I: Pathology for the health-related professions, ed 4, St. Louis, 2012, Saunders.
There is no known cause of JA. For some types of JA, there may be a genetic predisposition for the condition. Signs and symptoms of JA depend on the specific condition. Most JA conditions cause pain, swelling, redness, and warmth in the joints. Some JA conditions may also cause issues with the eyes, muscles, digestive system, and the skin.
The provider will perform an examination and order lab work, though no specific blood test diagnoses JA. The goal of the treatment is to provide the child with the best quality of life; therefore, pain control and reducing inflammation are important. A combination of medications, physical therapy, and nutrition therapy may be used.
Lyme Disease and Arthritis
Learning Objective: Discuss Lyme disease and arthritis, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Lyme disease is the most common tick-borne infectious disease in the United States. Lyme disease can cause flu-like symptoms and a rash (FIGURE 20.16A). If the infection is not treated, about 60% of people develop Lyme arthritis.
Lyme disease is caused by the bacterium Borrelia burgdorferi and, rarely, Borrelia mayonii in the United States. Infected deer and western black-legged ticks transmit the bacteria that cause Lyme disease (FIGURE 20.16B). This bacterial infection is prevalent in Wisconsin, Minnesota, California, and between Virginia and Maine. Exposure to grassy and heavily wooded areas increases the risk of coming in contact with infected ticks. Early signs and symptoms of Lyme disease include flu-like symptoms (fever, chills, achiness, fatigue, swollen lymph nodes, and headache) and a rash (erythema migrans). The rash appears about 70% to 80% of the time, usually starting 3 to 30 days after the bite. The rash begins at the bite site and slowly expands over the skin, reaching up to 12 inches or more. It can appear as a bull’s-eye or target.
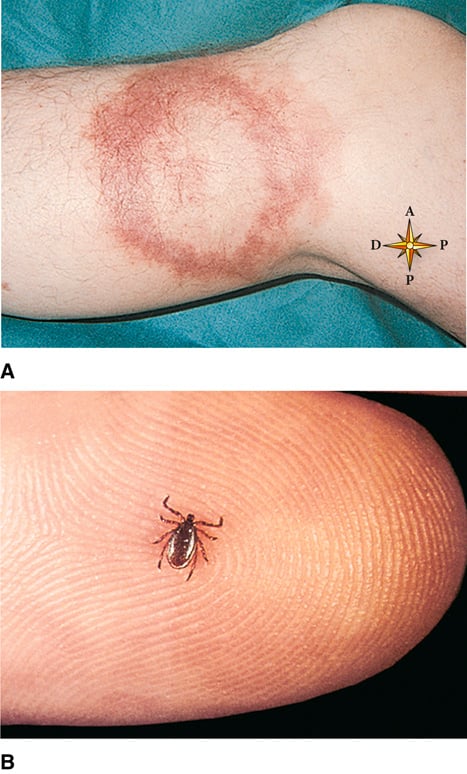
FIGURE 20.16 Lyme disease. (A) Circular, expanding rash resembling a bull’s-eye target caused by the spirochete bacteria Borrelia burgdorferi. (B) Deer tick, vector for transmission of Lyme disease. A: From Callen JP, Paller AS, Greer KE, et al: Color atlas of dermatology, ed 2, Philadelphia, 2000, WB Saunders; B: From Habif TP: Clinical dermatology, ed 5, St. Louis, 2010, Mosby.
If left untreated, Lyme disease can cause arthritis, severe joint pain, meningitis, Bell palsy, facial palsy (affecting both sides of the face), numbness and weakness in the extremities, heart palpitations (Lyme carditis), short-term memory issues, and eye inflammation.
After an examination, the provider will order an enzyme immunoassay (EIA) or immunofluorescence assay (IFA) blood test. If the results are positive or equivocal, further testing with IgM and/or IgG Western blot will be done. The lab test results are more reliable if a person has been infected for several weeks. Treatment includes antibiotics, such as amoxicillin, cefuroxime, and doxycycline. Some people may have post-treatment Lyme disease syndrome, which will resolve in time.
Patient Education for Lyme Disease
According to the Centers for Disease Control and Prevention (CDC), patient education for Lyme disease includes the following instructions:
• Minimize the risk for ticks in your yard by clearing tall grass, leaves, and brush.
• Treat clothing, boots, and camping gear with 0.5% permethrin.
• Use Environmental Protection Agency (EPA)–registered insect repellents. They contain DEET, picaridin, IR3535, Oil of Lemon Eucalyptus, para-menthane-diol (PMD), or 2-undecanone. You can also use the information found at the EPA website, www.epa.gov/insect-repellents/find-repellent-right-you.
• Wear pants tucked into socks and long-sleeved shirts when walking in wooded or grassy areas.
• Walk in the center of trails and avoid wooded and high-grass areas.
• Deer ticks are no bigger than the head of a pin. After you come indoors, check your entire body and your clothing, gear, and animals for ticks. Showering within 2 hours of potential exposure can reduce the chances of Lyme disease.
• If a person has a tick embedded, it needs to be removed. Wear gloves if possible. Use fine-tipped pointed tweezers. Get as close to the head as possible. Do not squeeze the abdomen because it may inject secretions into the person’s body. Pull upward with steady pressure to pull out the head. Once the tick is removed, place it in a container of rubbing alcohol to kill it. Clean the site with antiseptic soap and water. Apply an antibiotic ointment. Monitor the site for infection or other complications.
• If you develop a rash or fever within several weeks of removing a tick, see your healthcare provider. Be sure to tell the provider about your recent tick bite and when the bite occurred.
• Do not assume you are immune. Lyme disease can occur in the same person more than once.
Additional Arthritic Joint Disorders
There are several other arthritic conditions:
• Ankylosing spondylitis: A type of hereditary inflammatory arthritis affecting the back and spine, usually occurring between 17 and 35 years of age. Causes low back pain and stiffness, especially at night and in the morning.
• Infectious arthritis: Also called septic arthritis. Arthritis is caused by a joint bacterial (Staphylococcus aureus), viral, or fungal infections. Causes pain, swelling in a joint, fever and chills.
• Patellofemoral arthritis: The articular cartilage on the underside of the patella wears down and becomes inflamed and causes pain in the front of the knee. It makes kneeling, squatting, and taking the stairs difficult. Caused by dysplasia and patellar fracture.
• Psoriatic arthritis: A chronic autoimmune disease that can occur with psoriasis. The etiology is unknown. It causes joint pain and stiffness, fatigue, swelling of hands and feet, skin rashes, and eye problems.