Closing Comments
April 11, 2024
Patient Coaching
After the medical assistant coaches a patient on a topic, it is important for the medical assistant to evaluate the patient’s learning. The medical assistant should encourage the patient to “teach back” the preparation instructions or information so that she or he can evaluate whether the patient has an accurate understanding of the directions. Any errors or misunderstandings can be clarified. The patient should have a copy of directions or information to take home.
Legal and Ethical Issues
The medical assistant’s responsibility is to assist the provider and act as the patient’s advocate. All information discussed between the patient and the provider and all testing procedures ordered and done must remain confidential. Confidentiality and trust are closely linked, and these two issues form the basis of a sound patient-provider relationship. The medical assistant is an important part of that relationship and can strengthen it through ethical, professional conduct.
Patient-Centered Care
When coaching patients about diagnostic procedures, it is important for the medical assistant to give the patient a list of supplies (e.g., laxatives, enemas) required for the preparation. Patients may even need directions on where to purchase the supplies. The medical assistant should encourage the patient to call if there are questions or concerns to complete the preparation directions. If the patient is not completely prepared, the procedure may not be able to be done and may need to be rescheduled.
Professional Behaviors
Diagnostic procedures and treatment protocols, especially medications, are constantly changing. The professional medical assistant must be committed to lifelong learning to keep up with the rapid changes in the medical field. Maintaining a current understanding of the human body, the disease process, and how specific GI system diseases are diagnosed and treated requires a willingness to learn and adapt over time. This commitment to lifelong learning is a crucial part of becoming a professional medical assistant.
Summary of Scenario
Keith has learned a lot from the gastroenterology outreach team. He was able to shadow at the hospital to see several diagnostic procedures. Keith realizes that he will be continually learning with the team. He looks forward to learning more about digestive diseases, diagnostic procedures, and treatments. With everything he has seen to this point, he feels excited about his medical assistant career.
Summary of Learning Objectives
1. Examine the anatomy of the gastrointestinal tract.
The gastrointestinal tract consists of a large, muscular tube that, with the help of hormones and enzymes, digests food. The GI tract includes the mouth, pharynx (throat), esophagus, stomach, small intestine, and large intestine. The small intestine is made up of the duodenum, jejunum, and ileum. The large intestine is made up of the cecum, ascending colon, transverse colon, descending colon, sigmoid colon, and rectum.
2. Examine the anatomy of the accessory organs.
The accessory organs include the salivary glands, gallbladder, liver, and pancreas. These structures secrete fluids into the GI tract, aiding in digestion.
3. Differentiate among digestion, absorption, and excretion.
After food is ingested, the following three processes occur:
• Digestion: The breakdown of food into chemical substances.
• Absorption: The passage of substances and liquids through the lining of the GI tract into the body fluids and tissues.
• Excretion: The elimination of indigestible materials and waste products of metabolism.
The chemical digestion of carbohydrates, proteins, and fats occurs.
• Carbohydrates: Saliva contains an enzyme called salivary amylase, which starts to break down complex carbohydrates. Pancreatic juices contain amylase, which breaks down carbohydrates into sugars. In the small intestine, brush-border enzymes (sucrase, lactase, and maltase) are found in the microvilli and help with the final breakdown of carbohydrates.
• Proteins: In the stomach, hydrochloric acid softens and breaks down proteins and other foods. Pepsin, an enzyme found in the gastric juices, breaks down proteins into polypeptides. Pancreatic juices contain trypsin and chymotrypsin, which break down proteins into amino acids.
• Fats: Bile from the liver is also secreted in the duodenum and emulsifies fats. Pancreatic juices contain lipase, which breaks down fats into fatty acids and glycerol.
4. Analyze the life span changes to the gastrointestinal system.
Changes in the GI system occur during the first years of life. During pregnancy, progesterone causes the smooth muscles to relax, which affects the digestive system. With age, the stomach empties slower. Aging does not affect nutrient absorption. Constipation is more common with aging.
5. Examine the diseases and disorders of the mouth, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Diseases and disorders of the mouth include orofacial clefts (cleft lips and cleft palates), cavities, gingivitis, herpetic stomatitis, leukoplakia, periodontal disease, and thrush. Refer to this chapter for more information on these diseases and disorders.
6. Examine the diseases and disorders of the esophagus and stomach, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Diseases and disorders of the esophagus and stomach include gastroesophageal reflux disease, hiatal hernia, peptic ulcers, pyloric stenosis, achalasia, Barrett esophagus, esophageal atresia, esophageal varices, cyclic vomiting syndrome, dumping syndrome, gastritis, gastroparesis, and hypochlorhydria. Refer to this chapter for more information on these diseases and disorders.
7. Examine the diseases and disorders of the intestines, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Diseases and disorders of the intestines include acute appendicitis, celiac disease, diverticulitis, foodborne illnesses, hemorrhoids, hernias, inflammatory bowel disease (e.g., ulcerative colitis and Crohn disease), intestinal obstructions, irritable bowel syndrome, anal fissure, anorectal abscess, bowel incontinence, fistula, gastroenteritis, Hirschsprung’s disease, intestinal ischemia and infarction, intestinal volvulus, intussusception, and small intestinal bacterial overgrowth. Refer to this chapter for more information on these diseases and disorders.
8. Examine the diseases and disorders of the accessory organs, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Diseases and disorders of the accessory organs include cholelithiasis, cirrhosis, hepatitis, jaundice in newborns, nonalcoholic fatty liver disease, pancreatitis, acute cholecystitis, mumps, primary biliary cirrhosis, hemochromatosis, sialoliths, and sialadenitis. Refer to this chapter for more information on these diseases and disorders.
9. Examine the cancers of the gastrointestinal system, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Cancers of the gastrointestinal system include cancers of the oral cavity, pharyngeal and laryngeal cancers, stomach cancer, pancreatic cancer, liver cancer, small intestinal cancer, and colorectal cancer. Refer to this chapter for more information on these cancers.
10. Examine the medical assistant’s role in examinations, diagnostic procedures, and treatments for gastrointestinal diseases and disorders.
When a patient describes and points to the location of the pain, the medical assistant must know the underlying organs that may be involved. TABLE 19.1 provides possible screening questions for common signs and symptoms.
TABLE 19.2 discusses the diagnostic procedures for gastrointestinal diseases and disorders, along with the patient coaching for the procedure. TABLE 19.3 describes the medical laboratory tests for gastrointestinal diseases and disorders, which includes a comprehensive metabolic panel, C-reactive protein test, fecal immunochemical test, guaiac fecal occult blood test, H. pylori test, hepatitis liver panel, liver function tests, multitargeted stool DNA test, ova and parasite examination, stool culture, and total bilirubin.
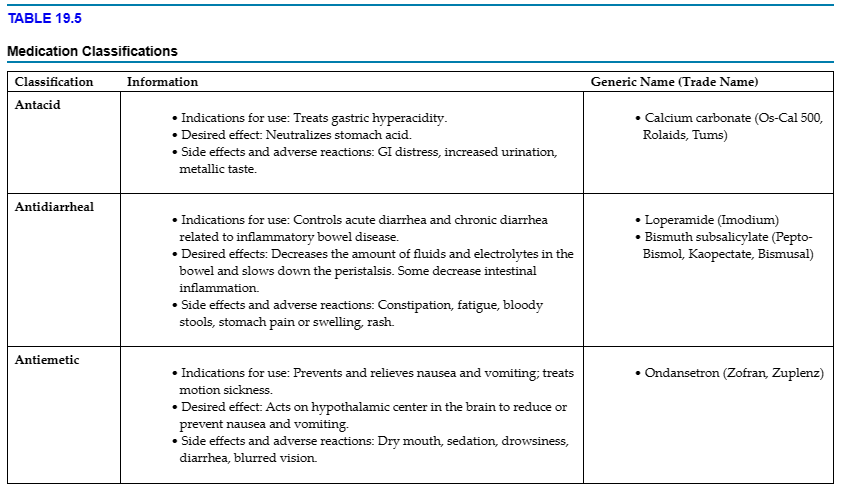
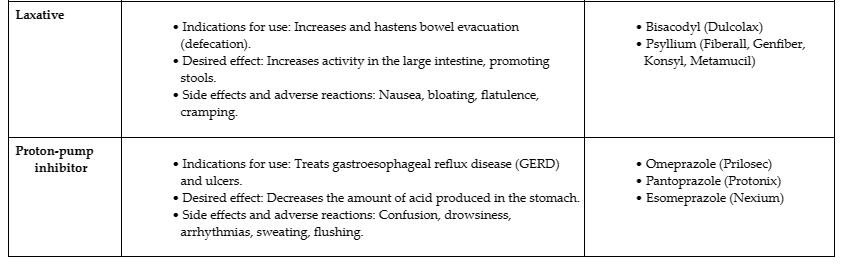
Common treatments used for gastrointestinal diseases and disorders are described in TABLE 19.4. The more common classifications of medications used for GI conditions include antacids, antidiarrheal, antiemetics, laxatives, and proton-pump inhibitors.
PROCEDURE 19.1 Use Critical Thinking When Performing Patient Screening
Tasks
Incorporate critical thinking skills when performing patient assessment. Document the patient’s history and chief complaint.
Scenario 1:
You work at Walden-Martin Family Medical (WMFM) Clinic. A patient calls and states that they have had nausea, vomiting, diarrhea, and abdominal pain for 3 days. You need to gather the patient’s information before talking with the provider, per the facility’s policy.
Scenario 2
You work at WMFM clinic. A patient calls and states that they have had vomiting and constipation for 4 days. You need to gather the patient’s information before talking with the provider, per the facility’s policy.
Directions
Role-play the scenario with a peer, who is the patient. Your instructor is the provider.
Equipment and Supplies
• Phone log and pen
• Patient’s health record
• Phone
Procedural Steps
1. Answer the telephone by the third ring, speaking directly into the mouthpiece or headset. Speak distinctly, using a pleasant tone and expression, at a moderate rate, and with sufficient volume.
PURPOSE:Answering promptly conveys interest in the caller. Proper positioning of the mouthpiece or headset allows for an audible tone.
2. Greet the caller, identify the facility and yourself, and offer to help the caller.
PURPOSE:Giving the facility’s name, in addition to the name of the staff member to whom the patient is speaking, lets the patient knows the correct number has been reached.
3. Verify the identity of the caller and the date of birth; access the patient’s record. Note the patient’s phone number in case you are disconnected.
PURPOSE:To have the patient’s health record ready for reference about the health history and recent care.
4. Determine the caller’s needs using therapeutic communication skills.
PURPOSE:To gather comprehensive information about the caller’s complaint and communicate empathetically about the caller’s needs.
5. Upon learning the patient’s complaint, use critical thinking skills and ask appropriate questions to obtain information about the patient’s condition for the provider. Identify the onset, frequency, and duration of the complaint. If related to pain, identify the exact location, quality (e.g., sharp, dull, stabbing), and rating (using a 0–10 pain scale). Identify significant history and factors that increase or decrease the complaint.
PURPOSE:Gathering relevant information helps the provider form an opinion on the patient’s care.
Scenario update: You know the provider is available, and the patient is willing to be put on hold as you talk with the provider.
6. Discuss the patient’s information with the provider. Present the information in an accurate, logical method.
PURPOSE:Presenting the patient’s information in a logical manner helps eliminate confusion and misunderstanding.
7. Upon returning to the phone, give the patient the information from the provider. Conclude the phone call.
8. Document the patient interaction, including the patient’s medical history, the provider notified, and the information relayed to the patient.
PURPOSE:For legal reasons, it is important to document all patient interactions.
PROCEDURE 19.2 Coach a Patient on Preparing for a Colonoscopy
Tasks
Coach a patient on the colonoscopy preparation. Document the coaching in the health record.
Scenario
You work at WMFM Clinic. You are working with Dr. David Kahn, who has asked you to coach Charles Johnson (DOB 03/03/19XX) on the colonoscopy patient instructions. Dr. Kahn wants Charles to take his antihypertensive medication the morning of the procedure, 1 hour after finishing the preparation solution.
The ambulatory surgical center requires that Charles not eat or drink anything starting at midnight on the day of the procedure. He needs to arrive 90 minutes before the procedure, which is scheduled for 11 a.m. He will be receiving IV sedation during the procedure and will need a driver to take him home.
Patient Instructions
Purpose of the colonoscopy:
• To detect abnormal changes in the large intestine and rectum.
Dietary preparations:
• Two days before the procedure: Do not take fiber supplements or eat foods high in fiber (e.g., nuts, seeds, whole grains, and raw or cooked fruits and vegetables).
• One day before the procedure: Do not eat solid foods; just drink clear liquids (e.g., broth, gelatin, coffee, tea, clear juice, popsicles, and sports drinks). Do not drink red liquids or eat red gelatin. Do not drink or eat dairy products or alcohol.
• On the day of the procedure: Do not eat solid foods or drink liquids other than the preparation solution from midnight onward.
Colon cleansing:
• Split the preparation solution (e.g., GoLYTELY, Colyte) and take half the evening before the procedure. Take the rest of the solution in the morning. The solution must be completed at least 2 hours before the procedure.
• Usually, within 1 hour of starting the preparation solution, liquid stools can occur and continue until 2 hours after completing the solution. Chills, headaches, cramping, weakness, nausea, vomiting, and bloating can occur when taking the solution. Drinking the preparation more slowly can reduce severe vomiting and cramping.
During the test:
• Sedation is usually given. You will be lying on your side on the exam table.
• The colonoscope will be inserted into your rectum. Air or carbon dioxide is pumped into the intestine to help the provider see the lining of the colon. This can cause some cramping.
• The procedure takes about 30 to 60 minutes.
After the test:
• You will need to recover about an hour after the test.
• Do not drive. Plan to have someone bring you home.
Directions: Role-play the scenario with a peer, who is the patient. Your instructor is the provider. Make up the location, date, and time of the procedure.
Equipment and Supplies
• Patient instructions
• Patient’s health record
Procedural Steps
1. Wash hands or use hand sanitizer.
PURPOSE:Hand sanitization is an important step for infection control.
2. Greet the patient. Identify yourself. Verify the patient’s identity with full name and date of birth. Explain what you will be doing in a manner that the patient understands. Answer any questions the patient may have.
PURPOSE:It is important to identify the patient in two different ways to ensure that you have the correct patient. Explaining the procedure can make the patient feel more comfortable and reduces anxiety.
3. Use simple language when talking. Speak clearly. Communicate with dignity and respect. Allow time for the patient to respond. Listen to the patient’s concerns.
PURPOSE:As with all patients, it is important to treat older patients with respect and dignity. Listening is important.
4. Ask if the patient has ever had a colonoscopy. If so, ask what the patient remembers about it.
PURPOSE:It is important to find out what the patient already knows about the topic.
5. Discuss the purpose of the colonoscopy and the preparation involved. Refer to the written instructions that the patient will be taking home.
PURPOSE:Referring to the written directions that will be sent home with the patient helps eliminate confusion.
6. Explain what the patient should expect during and after the procedure.
PURPOSE:Explaining what to expect during and after the procedure will reduce the patient’s anxiety about the procedure.
7. Ask the patient to teach back the preparation to you. Clarify any misconceptions or inaccuracies. Answer any questions the patient may have. Give a phone number to call the patient has questions.
PURPOSE:Using the teach-back method to evaluate the patient’s understanding will help identify any misunderstandings the patient may have.
8. Let the patient know when to anticipate the results. Also, give the patient the appointment information for the procedure, including the location, date, and time.
PURPOSE:Letting patients know when to expect test results helps alleviate confusion and anxiety.
9. Document the coaching in the patient’s health record. Include the provider’s name, what was taught, how the patient responded, and any written directions (including appointment information) sent home with the patient.
PURPOSE:It is important to document the procedure in the health record to show it was done.
Documentation Example08/14/20XX 1105 Per Dr. Kahn’s order, instructed pt on the colonoscopy preparation. Patient taught back the instructions accurately. Gave the patient the “Colonoscopy Patient Directions” booklet. Pt was notified of appointment on 08/25/20XX at 11 a.m. at AnyTown Surgical Center. ————————————————————————————————————————– Keith Williams, CMA (AAMA)