Ear Diseases and Disorders
April 11, 2024
Ear Diseases and Disorders
Learning Objective: Examine the diseases and disorders of the ear, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
The following sections discuss the common diseases and disorders of the ear, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Hearing Loss
Learning Objective: Discuss hearing loss, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Two problems result in hearing loss, a conduction problem and a sensorineural impairment. Some individuals have both conditions.
Conductive hearing loss is caused by a problem originating in the external or middle ear that prevents sound vibrations from passing through the external auditory canal, limits the vibration of the tympanic membrane, or interferes with the passage of bone-conducted sound in the middle ear. Some common causative factors in conductive hearing loss include impacted cerumen; trauma to the tympanic membrane, especially scar formation; hemorrhage or fluid in the middle ear; otosclerosis; and recurrent chronic ear infections. Patients with conductive hearing loss receive the greatest benefit from a hearing aid. If the hearing loss is caused by a malfunction or congenital abnormality of the ossicles, a surgical procedure can be performed to replace the damaged ossicles with manufactured models.
A sensorineural hearing loss results from an abnormality of the organ of Corti or the auditory nerve. Viral infection (e.g., rubella, influenza, herpes) can result in hearing loss, as can head trauma or certain ototoxic medications. The first sign of ototoxic drug complications usually is tinnitus. This sometimes occurs with high doses of aspirin, certain antibiotics (erythromycin and vancomycin), and chemotherapeutic agents. A sensorineural hearing loss also can occur because of prolonged exposure to loud noise, such as repetitive noise in the workplace, or loud music, which damages the delicate cilia lining the organ of Corti.
Presbycusis, the hearing loss that affects older adults, is caused by a reduction in the number of receptor cells in the organ of Corti and is also classified as a sensorineural loss. Children can be born with a congenital hearing deficit or deafness because of an intrauterine infection, such as measles (rubella) (Figure 16.9).
If the sensorineural hearing loss cannot be improved by hearing aids, an option is surgical insertion of cochlear implants. These are complex devices that use electrical impulses to stimulate the auditory nerve, which carries the current to the brain to be interpreted as sound. Cochlear implants bypass damaged portions of the ear and directly stimulate the auditory nerve. These implants do not create normal hearing but provide increased sound for a person with profound or complete hearing loss.
Mixed hearing loss is a combination of conductive and sensory deafness. This type of loss can result from tumors, toxic levels of certain medications, hereditary factors, and stroke.
Otitis
Learning Objective: Discuss otitis, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
There are two common types of otitis. The first affects the external ear canal and is called otitis externa or swimmer’s ear. Otitis externa may be caused by dermatologic conditions, such as seborrhea or psoriasis, trauma to the canal, or continuous use of earplugs or earphones. Swimmers frequently have otitis externa because water collects in the ears and mixes with cerumen to form an ideal culture medium for bacteria and fungus. Patients with otitis externa complain of severe pain and have inflammation and swelling of the external auditory canal, hearing loss, and possibly purulent (containing pus) or serous drainage. The inflammation is treated with antibiotic or steroid eardrops, and the canal must be kept clean and dry, or the condition can become chronic.
Otitis media is an inflammation of the normally air-filled middle ear that results in a collection of fluid behind the tympanic membrane. Otitis media can be serous (otitis media with effusion [OME]) or suppurative. Serous otitis media occurs because of a buildup of clear fluid in the middle ear; patients complain of a full feeling and some hearing loss. In suppurative otitis media, purulent fluid is present in the middle ear, and the patient has fever, pain, and hearing loss. Otitis media often is associated with an upper respiratory tract infection caused by a virus or an allergic reaction that results in swelling and inflammation of the sinuses and eustachian tubes. A child’s eustachian tube is shorter, narrower, and more horizontal than that of an adult. The small size and decreased angle for drainage increases the chance that inflammation will block the tube and cause fluid to collect in the middle ear, which not only is uncomfortable but also interferes with the conduction hearing process (Figure 16.10).
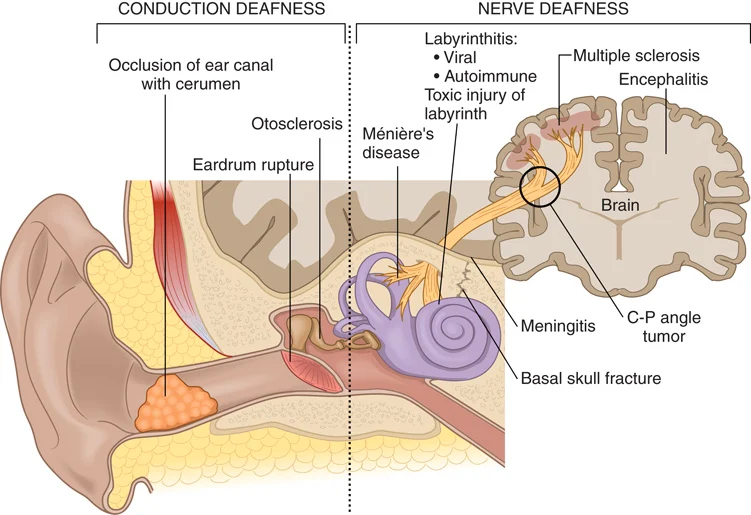
FIGURE 16.9 Causes of deafness.
Risk Factors for Otitis Media
Factors That Cannot Be Controlled
• Sex (male)
• Age (infants and younger children [6 to 18 months])
• Premature birth
• Family history
• Siblings with infections
• Seasonal factors (most common during cold and flu season), seasonal allergies
• Underlying disease (cleft palate, Down syndrome, asthma, allergies)
• Ethnicity (Native American and Alaskan Inuit because of the shape of the eustachian tubes)
• Cochlear implants
Factors That Can Be Controlled
The following behaviors can lower a child’s risk for otitis media:
• Limit exposure to large-group child care settings.
• Do not expose the child to second-hand smoke.
• Hold the child upright during bottle feeding.
• Do not use pacifiers beyond 6 months, which may increase the risk.
• Wash hands frequently to prevent the spread of colds and flu.
• Have the child immunized with the pneumococcal conjugate vaccine (Prevnar) and the flu vaccine.
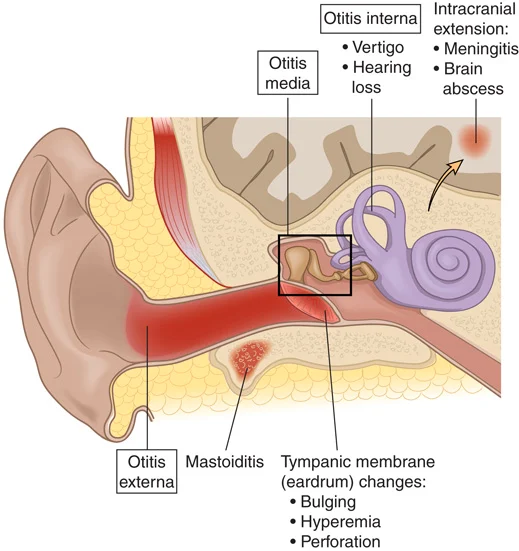
FIGURE 16.10 Inflammation and infection of the ear and surrounding tissues.
An otoscopic examination reveals that the normally pearly gray tympanic membrane is inflamed (bright pink or red) and bulging (Figure 16.11). Areas of fluid or pus may be visible through the membrane. A tympanogram may be done to determine the air pressure of the middle ear and the mobility of the tympanic membrane. During a tympanogram test, a small earphone is placed into the ear canal, and the air pressure is gently changed. This test is helpful in showing whether an ear infection or fluid is present in the middle ear (Figure 16.12). A tympanic membrane responding normally to an increase in air pressure will move, resulting in a peaked tympanogram. If fluid or pus in the middle ear is putting pressure on the tympanic membrane, the membrane moves only slightly or not at all, resulting in a slight peak or a flat tympanogram recording.
Treatment of otitis media may be a conservative “watch and wait” approach. However, if a fever and pronounced pain are present, the individual may be given antibiotics and told to take over-the-counter analgesics such as acetaminophen or ibuprofen. If this condition becomes chronic, the provider may recommend a myringotomy, which is the creation of a surgical incision in the tympanic membrane to drain the fluid, followed by the insertion of a tympanostomy tube to continually drain the middle ear of fluid. This may be necessary to prevent permanent hearing loss caused by damage to the ossicles (Figure 16.13).
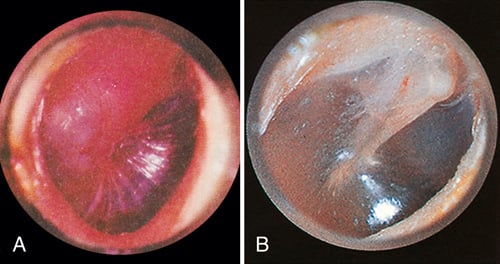
FIGURE 16.11 (A) Tympanic membrane with otitis media. (B) Normal tympanic membrane. From LaFleur Brooks M: Exploring medical language, ed 9, St. Louis, 2014, Mosby.
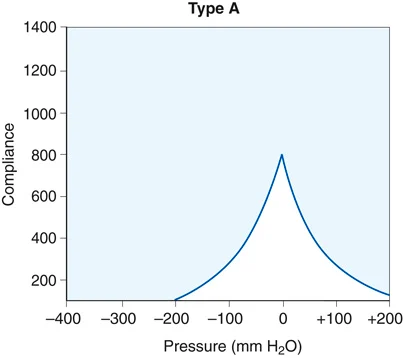
FIGURE 16.12 A normal tympanogram shows a peak at normal pressure (0). An ear with fluid produces a flat tympanogram.

FIGURE 16.13 Tympanic membrane with a tympanostomy tube. From Frazier MS, Drzymkowski JW: Essentials of human diseases and conditions, ed 5, St. Louis, 2013, Saunders.
Recommendations for Treating Otitis Media
The development of drug-resistant strains of bacteria due to overprescribed antibiotics is a growing concern. The American Academy of Pediatrics recommends the following for the treatment of otitis media:
• Treatment with antibiotics should be delayed, giving the child’s immune system a chance to fight the infection by itself. This delay should last 24 hours in children 6 to 24 months old and 72 hours for older children. Approximately 61% of children improve within 24 hours, regardless of whether they are treated. If the child’s condition does not improve, an appropriate antibiotic can be prescribed.
• The child typically improves within 48 to 72 hours, but the parent should understand how important it is to complete the antibiotic medication as ordered to prevent the infection from recurring.
• The provider may decide to treat otitis media with a short course of antibiotics (i.e., 5 days) but at a higher dose. The drugs of choice include amoxicillin (Amoxil), azithromycin (Zithromax), and cefuroxime (Rocephin).
• Antibiotics will not help if otitis is caused by a virus. The child should be observed for possible complications, and analgesics should be administered for pain control. Viral otitis media typically resolves within 7 to 14 days.
Medical assistants play a key role in helping parents understand why antibiotic therapy may not be recommended. They also must educate parents about the importance of administering a prescribed antibiotic at the time ordered, using the correct dose, and completing the entire prescription.
Impacted Cerumen
Learning Objective: Discuss impacted cerumen, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Cerumen normally is a soft, yellowish, waxy substance that lubricates the external auditory canal. Impacted cerumen that has been pushed up tightly against the eardrum is a common cause of conductive hearing loss because sound vibrations cannot pass through the cerumen to initiate movement of the tympanic membrane. Individuals with psoriasis, abnormally narrow ear canals, or an excessive amount of hair growing in the ear canals are more prone to this condition. Excessive secretion of cerumen can gradually cause hearing loss, tinnitus, a feeling of fullness, and otalgia (ear pain).
An otoscopic examination quickly reveals this problem. If impacted cerumen is found, it must be removed. This can be done by softening the wax with oily drops, such as carbamide peroxide (Debrox), and then irrigating the ear with warm water until the plug is removed. Because this condition can recur, the patient may need to schedule periodic examinations. If the patient is experiencing hearing loss because of the impaction, it is immediately remedied with the removal of the cerumen.
Ménière Disease
Learning Objective: Discuss Ménière disease, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Ménière disease is a disorder of the inner ear. It is characterized by vertigo, tinnitus, progressive hearing loss, and sometimes a feeling of pressure or fullness in the ear. It usually only affects one ear. The cause of Ménière disease is not well understood. The inner ear of persons with this condition seems to have an abnormal amount of fluid (endolymph). What causes the excess fluid is not known. Research indicates the following possible causes: abnormal anatomy of the inner ear, genetic predisposition, possible autoimmune condition, head trauma, or migraines.
Ménière disease causes swelling and edema in an endolymphatic sac of the semicircular canals, along with an overproduction or collection of excess endolymph. When an acute attack occurs, the patient may experience nausea, vomiting, and problems with balance. These attacks can last a few hours to several days, and they may increase in severity over time. Although the cause of this problem is unknown, Ménière disease is a chronic, progressive condition that triggers episodes of recurring attacks of vertigo, tinnitus, a sensation of pressure in the affected ear, and advancing hearing loss.
During active periods of the disease, the patient is treated symptomatically with medications for nausea and vomiting. A salt-restricted diet, diuretics, and antihistamines may be prescribed to control edema in the labyrinth of the inner ear. Surgical destruction of the affected labyrinth is an option. Although this relieves symptoms, it may also result in permanent deafness if the cochlea is damaged.