Hematology in the Physician Office Laboratory
April 11, 2024
Learning Objective: Examine the hematology tests, including the erythrocyte sedimentation rate and coagulation testing, done in the physician’s office laboratory.
Hematology testing can occur in the POL or at a reference laboratory. For many POL hematology tests, an adequate blood sample can be obtained from a capillary puncture of the finger. If a larger sample is required, blood can be obtained via venipuncture.
Hematology tests done in the physician’s office laboratory can include the erythrocyte sedimentation rate, coagulation tests, and a complete blood count. These tests are described in the following sections.
Erythrocyte Sedimentation Rate
Learning Objective: Describe an erythrocyte sedimentation rate test.
The erythrocyte sedimentation rate (ESR) is a laboratory test that measures the rate at which red blood cells gradually separate from plasma and settle to the bottom of a specially calibrated tube in 1 hour.
The ESR is not specific for any disease in particular but is used as a general indicator of inflammation. ESR and C-reactive protein (CRP) testing should correlate as indicators of inflammation. Normal values for males under age 64 are 0 to 15 mm/hr. Normal values for males over 64 and females are 0 to 20 mm/hr. A lower-than-normal ESR is not considered clinically significant. An increased ESR is significant to the provider because it indicates the presence of inflammation in the body. An increased ESR is seen in several conditions:
• Acute and chronic infections, such as tuberculosis and hepatitis
• Autoimmune conditions such as rheumatoid arthritis, lupus erythematosus, and rheumatic fever
• Multiple myeloma and other types of cancers
Several CLIA-waived methods of measuring the ESR are used, including the Sediplast procedure (Procedure 34.1). This closed system incorporates a pierceable stopper that ensures a leakproof seal when punctured by a pipet. An automatic self-zeroing cap and reservoir accurately bring the blood level to the zero mark and prevent overfilling. A prefilled vial of sodium citrate reagent is provided for dilution of blood before testing. A closed-tube Streck ESR method uses a Streck black-topped Vacutainer sample of blood that is directly placed in a Streck rack that provides results in 30 minutes (FIGURE 34.1).
Many factors can affect the ESR. The tube must be filled with blood and must not have air bubbles. The tube must be allowed to sit in a vertical position, undisturbed, for the full designated time—careful timing is important. Tilting a tube even slightly may increase the sedimentation rate. Jarring or vibrations from nearby machinery will falsely increase the ESR.
Coagulation Testing
Learning Objective: Describe coagulation testing and related patient education.
Coagulation testing is used when a patient has a blooding disorder or when a patient is taking an anticoagulant, such as warfarin. Patient education is important to help patients regulate their coagulation test results when taking anticoagulants.
Prothrombin Time
Prothrombin time (PT or protime) is a blood test that measures the time it takes for the plasma of your blood to clot. PT test results are reported as the number of seconds blood takes to clot when mixed with the thromboplastin reagent. Prothrombin is a protein found in plasma that is converted to thrombin as part of the clotting process. Thrombin then causes fibrinogen to be converted to fibrin during the clotting process.
The normal range for a PT result is 11 to 13.5 seconds. A number lower than the normal range means the blood clots more quickly than normal, and a higher number means it takes longer for the blood to clot. Taking vitamin K supplements or estrogen-containing medications (e.g., oral contraceptives and hormone replacement medications) or eating foods high in vitamin K can cause the blood to clot too quickly. This means it decreases the clotting time or lowers the PT numeric value. Blood that clots too slowly can be caused by anticoagulant medication, liver disease, vitamin K deficiency, and clotting factor deficiencies.

FIGURE 34.1 30-minute Streck ESR CLIA-waived test.
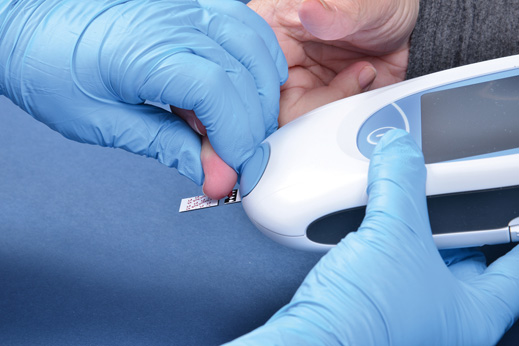
FIGURE 34.2 Applying a blood sample to the CoaguChek XS PT test monitor.
CLIA-waived tests for professional and home use are available for testing the PT. This test can be performed using a handheld, CLIA-waived instrument that uses whole blood from a fingerstick (FIGURE 34.2). The CLIA-waived CoaguChek XS PT measures the time it takes a blood sample to form a fibrin clot. A precise amount of capillary sample blood is dispensed into the channels of a testing strip. The blood is mixed with a thromboplastin reagent. The blood is pumped back and forth in the channel, and a series of light-emitting diodes (LEDs) detect the formation of a clot when blood movement in the channels stops (Procedure 34.2).
The PT is often used in combination with the partial thromboplastin time (PTT) to screen for hemophilia and other clotting disorders. The PT is also used to monitor patients taking anticoagulant drugs such as warfarin and similar anticoagulants. Warfarin is given to prevent clots in deep veins of the legs and to treat a pulmonary embolism.
International Normalized Ratio
The PT test results can vary by laboratory based on the thromboplastic reagent used. To standardize the reporting, the World Health Organization (WHO) created the international normalized ratio (INR). The INR is a conversion unit that considers the different sensitivities of reagents. It is widely accepted as the standard unit for reporting PT results rather than the actual clotting time.

FIGURE 34.3 Warfarin flow sheet.
The normal PT values are 11 to 13.5 seconds or an INR of 0.8 to 1.1. Each increase in the INR of 0.1 means the blood is slightly thinner; thus it takes longer to clot. Patients who are taking warfarin to prevent the formation of blood clots or who have artificial heart valves should have an INR value of about 2.0 to 3.0. Their blood should take longer to clot than that of a normal healthy individual. An INR result higher than 3.0 puts a person at even higher risk of bleeding, and a result lower than 2.0 puts a person at risk of developing a blood clot.
The medical assistant needs to know how to accurately document INR follow-up and related warfarin dosages on a patient flow sheet. The provider will balance repeated INR levels with the warfarin dosage, so the INR is maintained at about 2.0 throughout the anticoagulant treatment (FIGURE 34.3).
Patient Education
Patient education is important when patients are being monitored with coagulation testing. Patients need to know the importance of the following:
• Follow-up testing: Patients who are taking the anticoagulant warfarin will need to follow up with the required lab work to monitor their PT/INR.
• Vitamin K intake: Vitamin K can increase blood clotting times. This means vitamin K works against the effects of warfarin. Helping patients identify foods high in vitamin K is crucial to maintaining a proper PT/INR value. Foods high in vitamin K include kale, mustard greens, Swiss chard, collards, spinach, brussels sprouts, broccoli, and beef liver. Most providers encourage patients to eat a consistent amount of vitamin K and not overindulge in foods high in vitamin K. A consistent level of vitamin K in the diet will help patients maintain consistent PT/INR results.
• Substances that can affect the PT/INR results: Drinking large amounts of alcohol (three drinks per day) or taking aspirin, heparin, antihistamines, antibiotics, and vitamin C can change the results. If a patient is taking warfarin, many medications and over-the-counter products can interact with the medication. For example, garlic and Gingko biloba can increase the risk of bleeding, whereas St. John’s wort and ginseng decrease the effects of warfarin. Patients should notify their providers of all prescribed and over-the-counter products they use.
PT/INR Home Monitoring
Some patients may need to monitor their PT/INR results at home. The PT/INR home monitors may be considered medically necessary durable medical equipment by the patient’s insurance company if the person is on oral anticoagulation therapy for a variety of conditions. The medical assistant may be responsible for assisting the patient with the paperwork that must be completed to obtain the monitor and for coaching the patient on how to perform the test.
When coaching the patient on the process, it is useful to have the home machine available. The medical assistant should discuss how to get a successful blood sample by warming a cold finger, cleaning the site, and not squeezing the finger. The medical assistant should teach the patient the process (see Procedure 34.2). Then the patient should provide a return demonstration to ensure the patient knows the steps.
Typically, patients need to test every 1 to 4 weeks. They may need to report the results to the provider through their online patient portal or upload the monitor’s history through the patient portal.
34.1 Critical Thinking Application
Anita just roomed Janine Butler. She has an appointment today, and Dr. Perez would like to check her PT/INR results. Janine is on warfarin, but her INR is still a bit low. Anita checked her chart, and the INR completed in the lab is 1.7. Is this an acceptable result for someone who is on medication to prolong clotting time? Is it too high, too low, or normal?