Pituitary Gland Disorders and Disorders
April 11, 2024
Learning Objective: Examine pituitary gland diseases and disorders, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Anterior pituitary gland dysfunction can lead to several diseases and disorders. Hypersecretion of growth hormone causes acromegaly and gigantism, whereas hyposecretion causes dwarfism. Hypersecretion of prolactin causes prolactinoma. Women with hyposecretion of prolactin are unable to maintain breast milk production. Hyposecretion of all the anterior pituitary hormones causes panhypopituitarism.
Posterior pituitary gland hypersecretion of ADH causes a syndrome of inappropriate antidiuretic hormone (SIADH), and hyposecretion causes diabetes insipidus. The following sections discuss the more common pituitary diseases.
Acromegaly
Learning Objective: Describe acromegaly, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Acromegaly is a rare condition with too much growth hormone in the body. It is seen after normal bone growth has stopped (end of puberty).
Acromegaly is caused when the pituitary gland makes too much growth hormone. Usually, a benign tumor in the pituitary gland releases too much GH. Acromegaly can cause the following:
• Excessive sweating and body odor
• Decrease in muscle strength, carpal tunnel syndrome, and joint pain and swelling
• Large bones of the face, jaw, feet, and hands (FIGURE 24.5)
• Hirsutism, high blood pressure, and weight gain
• Decreased peripheral vision, headache, hoarseness, and sleep apnea
After a medical history and physical, the provider will order laboratory tests, including those used to analyze blood glucose, growth hormone and growth hormone suppression, insulin-like growth factor 1, and prolactin. A magnetic resonance imaging (MRI) scan of the brain and a spinal x-ray may be ordered, along with an echocardiogram, colonoscopy, and sleep study. Treatment consists of surgery to remove the tumor, radiation, and medication to block GH production. Follow-up visits are usually required to ensure that acromegaly does not come back.
Gigantism
Learning Objective: Describe gigantism, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Gigantism is a rare condition in which there is too much growth hormone in the body during childhood.
Gigantism is caused when the pituitary gland makes too much growth hormone. Usually, a benign tumor of the pituitary gland releases too much GH. Rare genetic diseases can also cause gigantism. The child will grow extremely large for his or her age (FIGURE 24.6). Additional signs and symptoms include the following:
• Delayed puberty and irregular periods (menstruation)
• Double vision, difficulty with peripheral vision, and voice changes
• Large hands and feet, thickening of facial features, and prominent forehead and jaw
• Joint pain, weakness, and gaps between teeth
• Increased sweating and headaches
After an examination, the provider will order laboratory tests, such as the following:
• Insulin-like growth factor -1 (IGF-1) level, growth hormone levels, and oral glucose tolerance test (OGTT)
• Cortisol and prolactin
• Estradiol (type of estrogen) for girls and testosterone for boys
• GH suppression test and thyroid hormone
A computed tomography (CT) or MRI scan of the head may also be done. Surgery can cure many cases. If the tumor cannot be completely removed, medications that suppress the GH release can be given.
Dwarfism
Learning Objective: Discuss dwarfism, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Dwarfism is also known as “short stature,” and someone with this condition may be called a “little person.” The person has a short stature or an adult height of under 4 feet 10 inches (58 inches) (FIGURE 24.7). Dwarfism does not affect intelligence. It can occur in families with average-height parents. There are two types of dwarfism:
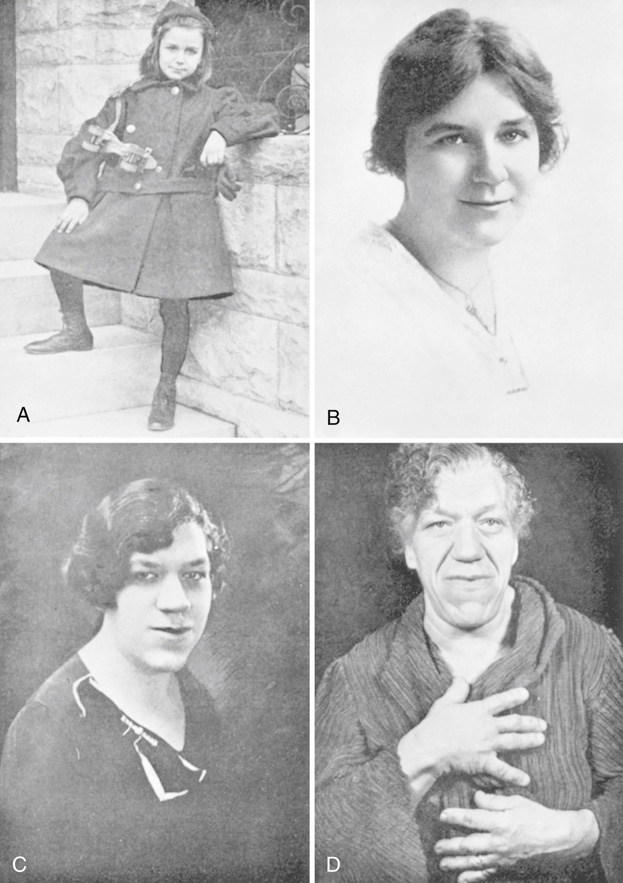
FIGURE 24.5 Progression of acromegaly. (A) Patient at age 9. (B) Patient at age 16, with possible early features of acromegaly. (C) Patient at age 33, with well-established acromegaly. (D) Patient at age 52, end-stage acromegaly. From Clinical Pathological Conference, Am J Med 20:133, 1956.

FIGURE 24.6 Gigantism. From Sainani GS, Joshi VR, Sainani RG: Manual of clinical & practical medicine, New Delhi, 2010, Elsevier India.
• Disproportionate dwarfism, which occurs when some parts of the body are small, whereas others are average or above-average size.
• Proportionate dwarfism, which occurs when the parts of the body are proportionate. Usually, medical conditions in early childhood that limit growth and development cause proportionate dwarfism.
Most types of dwarfism are caused by a genetic mutation. There are more than 300 different conditions that cause dwarfism, with achondroplasia being the most common. Achondroplasia, a genetic condition, causes the arms and legs to be short compared to the head and trunk. Metabolism problems, hormones, kidney disease, and other genetic conditions can also cause dwarfism. Besides a short stature, the signs and symptoms vary based on the condition causing the dwarfism. People with disproportionate dwarfism may have the following characteristics:
• Short fingers, arms, and legs; limited mobility at the elbows; bowed legs; and swayed lower back
• Average-size trunk
• Disproportionately large head with a prominent forehead

FIGURE 24.7 The normal 3-year-old boy is in the 50th percentile for height. The short 3-year-old girl exhibits the characteristic “kewpie doll” appearance, suggesting a diagnosis of growth hormone deficiency (GHD). From Zitelli BJ, Davis HW: Atlas of pediatric physical diagnosis, ed 5, St. Louis, 2007, Mosby.
People with proportionate dwarfism have a height below the third percentile on growth charts. Their growth rate is slower than expected for their age. Sexual development is delayed or absent during the teen years.
Dwarfism can be diagnosed during pregnancy or early in life as the child’s growth slows. Measurements and appearance, along with imaging technology (e.g., x-rays), genetic testing, and hormone tests, are used. Treatment is focused on maximizing functioning and independence. Most treatments do not increase the stature but rather correct problems caused by complications. For some patients, growth hormone therapy can be given to help increase stature. Daily injections may be needed for several years until the child stops growing.
Diabetes Insipidus
Learning Objective: Describe diabetes insipidus, including the signs, symptoms, etiology, diagnostic procedures, and treatments.
Diabetes insipidus (DI) is caused by a hyposecretion of ADH. The hypothalamus does not produce enough of the hormone, or the posterior pituitary gland does not release a sufficient amount of it.
There are several types of DI, and the causes vary, including genetics, a tumor, trauma, or pituitary gland surgery. Diabetes insipidus can also occur if there is an inadequate response to ADH in the renal tubules of the nephrons due to kidney disease or certain medications. The signs and symptoms usually have an acute onset and include the following:
• Polydipsia, polyuria, nocturia (frequent urination at night), and very dilute urine
• Trouble sleeping, fussiness, and irritability
• Fever, vomiting, diarrhea, and hypotension (low blood pressure)
• Delayed growth and weight loss in children
Complications, such as hypernatremia (abnormally high blood sodium level), severe dehydration, electrolyte imbalance, and hypotension may occur.
The provider will do a physical exam and may order laboratory tests, including a urinalysis and blood tests. A water deprivation test and imaging tests can also be done. Diabetes insipidus can be fatal if not adequately treated. Treatment focuses on the cause of the condition. Medications such as a synthetic ADH hormone (desmopressin [DDAVP]) and diuretics may be given.
Additional Pituitary Gland Disorders
Learning Objective: Describe additional pituitary gland disorders.
Additional pituitary gland diseases include the following:
• Prolactinoma: A benign tumor of the pituitary gland that causes the hypersecretion of prolactin. Women have abnormal lactation and abnormal menstrual cycles. Men experience impotence.
• Panhypopituitarism: Caused by the hyposecretion of all anterior pituitary hormones, which results from the destruction or deficiency of the entire anterior lobe. It is most common in women. It causes hypotension, weight loss, weakness, and loss of libido.
• Syndrome of inappropriate antidiuretic hormone (SIADH): Caused by the hypersecretion of ADH. SIADH causes an inability to produce and secrete diluted urine. Water retention, hyponatremia (a low blood sodium level), and weight gain are seen.
24.3 Critical Thinking Application
Cecilia is working with Landon, who was just diagnosed with diabetes insipidus. Landon’s mother asks Cecilia how often he would need to take insulin. How would you address this question? Could you, as a medical assistant, correct the mother’s misconception about diabetes insipidus?