Reproductive Issues
July 2, 2023
Recovery Stage
Check the fundus and lochia every 15 minutes for the first 1 or 2 hours after delivery. The fundus should remain contracted, firm, and midline. This is critical because severe bleeding may result if the uterus does not tightly constrict the placental site. A full bladder can displace the uterus and prevent its contraction. Encourage the patient to empty her bladder before checking the fundus. Palpate the uterus by placing one hand over the lower segment of the uterus near the pubic bone. Use the side of the other hand to feel the location and consistency of the uterus (see Figures 26-8 and 27-1).
If the fundus is not firm, it may be difficult to locate. An atonic uterus, one that has lost muscle tone, feels soft or boggy. Gently massage the fundus to increase contractility. Small clots frequently are expressed during this maneuver, and the uterus regains good contracted tone. If this does not result in contraction, the primary care provider should be notified. Oxytocic medications may be prescribed. Examples include oxytocin (Pitocin) and methylergonovine maleate (Methergine). These are usually administered intravenously to obtain prompt response. Methylergonovine may also be administered intramuscularly or orally. Monitor vital signs closely if these medications are given because they may cause elevated blood pressure, bradycardia, nausea, headache, vertigo, and other side effects (Table 27-3).
While palpating the uterus, observe the amount of lochia. If the uterus is contracting well, small to moderate amounts of drainage are observed. If tone is poor, the amount of lochia is increased. Learn what amount is considered scant, light, moderate, and heavy. This is usually determined by the number of absorbent pads saturated in a period, such as pads per hour (Figure 27-4). The time factor is important when assessing lochia. One pad saturated in 30 minutes is more serious than one pad saturated in 4 hours. Pay particular attention to the patient who has a small but steady trickle of lochia; the blood loss may be significantly greater than in those who seem to bleed larger amounts (see Table 27-1). Also, be sure to check under the buttocks of the patient who remains in the supine position; many times gravity causes drainage to miss the pad and pool under the patient.
Later Postpartum Stage
Perform daily assessments of the breasts, the fundus, lochia, the perineum, the rectum, and the vascular condition of the legs.
As in the recovery stage, assess the location and consistency of the uterine fundus for the normal signs of involution. It is normally located at the level of the umbilicus on the day of delivery. The first day postpartum it may be one fingerbreadth above or at the level of the umbilicus; after that, it normally descends at the rate of one fingerbreadth per day (see Figure 27-1, A). When assessing the fundus of a woman who delivered via cesarean, carefully palpate the sides of the incision to determine uterine tone and position.
As during the early recovery stage, the fundus should remain firmly contracted. Manage any atony as described. If massage does not result in adequate contraction, notify the physician. Lochia may begin to change within the first 2 days from the rubra to the serosa form. Assess the amount of drainage. Frequently, less lochia is observed after cesarean deliveries because the uterine cavity is suctioned as part of the surgical procedure. The odor of the lochia should remain fleshy. If a fetid odor is detected, infection may be present; report this promptly.
Inspect the perineum and the rectum by having the woman assume a lateral position with the upper leg drawn toward the chest. The perineum should be approximated. If an episiotomy was performed, the tissue may appear edematous. Erythema is common. Ecchymosis is also common, particularly after a difficult delivery. Many physicians order some form of topical anesthetic, such as witch hazel (Tucks pads) or dibucaine (Nupercainal) ointment, to soothe the perineum (see Table 27-3). This should be applied to the perineum with a clean, lint-free tissue, not the fingers.
If localized edema, discoloration, and intense pain are observed in the perineal area, a hematoma may be present. This hematoma is caused by excessive bleeding into the tissue. A hematoma is most common after deliveries in which forceps were used. Hematomas may be obvious or may be concealed in the vaginal canal. If the woman reports persistent perineal pain or fullness in the vagina, notify the physician. This problem necessitates medical attention and perhaps surgical intervention.
Although the rectum and legs are not part of the reproductive system, these areas are typically included
Table 27-3 Medications for the Mother and Newborn
GENERIC NAME (TRADE NAME) | ACTION | SIDE EFFECTS | NURSING IMPLICATIONS |
codeine (with acetaminophen; Tylenol #3) oxycodone terephthalate (with acetaminophen; Percocet) | Pain reliever, narcotic | Drowsiness, sedation, nausea, vomiting, constipation, respiratory depression, urinary retention, allergic reactions, rash, urticaria | Avoid concomitant use of alcohol or other central nervous system–depressant drugs; tell patient to avoid driving or other hazardous tasks while taking these medications; warn patient that extended use may result in dependency; avoid overdosing mother on acetaminophen. |
ibuprofen (Advil, Motrin, Nuprin) | Nonsteroidal anti-inflammatory with antipyretic and analgesic properties | Heartburn, nausea, pruritus, lightheadedness, gastrointestinal bleeding | Give 1 hr before or 2 hr after meals; with gastrointestinal intolerance, give with meals; instruct patient to avoid taking aspirin or acetaminophen concurrently; teach patient to avoid alcohol intake and to report gastrointestinal distress or bleeding. |
methylergonovine maleate (Methergine) | Oxytocic agent, stimulates uterine contraction, used to control postpartum bleeding | Headache, dizziness, nausea, chest pain, tachycardia, hypertension | Contraindicated in patients sensitive to ergot derivatives. |
oxytocin (Pitocin) | Oxytocic agent, stimulates uterine contractions | Mother: nausea, vomiting, uterine spasm or rupture, water intoxication, seizures, cardiac arrhythmias, hypotension Fetus: cardiac arrhythmias, central nervous system or brain damage | Carefully monitor intake and output; fetal heart tones; and length, duration, and force of uterine contractions. |
simethicone (Mylicon) | Antiflatulent | None | Instruct patient to chew tablet thoroughly before swallowing; give after meals. |
Rho(D) immune globulin (RhoGAM) | Gamma globulin solution containing immunoglobulins (IgG); provides passive immunity by suppressing antibody response and formation of anti-Rh(D) in Rh-negative individual exposed to Rh-positive blood | Injection site irritation; slight fever and lethargy | Check lot number, administer IM only to mother, using deltoid muscle within 72 hr of pregnancy termination. |
rubella vaccine | Live virus vaccine | Rash, joint pain, pain at site Does not harm breastfeeding mothers | Administer IM in deltoid muscle during postpartum period; warn patient to avoid pregnancy for at least 3 mo. Obtain informed consent. |
Vitamin, prenatal (Materna) | Vitamin supplement | Nausea, vomiting | Tell patient it is important that pregnant women take prenatal vitamins and not regular vitamin supplements and that prenatal vitamins contain extra folic acid, which is needed for normal fetal development. |
Witch hazel (Tucks pads, cream) | Astringent | Local irritation | Instruct mother that it is for external use only; use for relief of perineal discomfort. |
dibucaine ointment (Nupercainal) | Topical anesthetic | Allergic reactions, burning, stinging | Instruct mother that it is for external use only (application to severely denuded tissue may result in systemic absorption). |
Vitamin K (AquaMEPHYTON) | Antidote for inadequate absorption and synthesis of vitamin K in neonate | With a large dose: hyperbilirubinemia, hemolytic anemia, kernicterus | Administer 0.5-1 mg IM in the middle third of the infant’s vastus lateralis muscle of thigh after delivery. Stabilize leg firmly. |
Purified lanolin cream | Retains the skin’s natural moisture and protects the mother’s nipple from further abrasions | None; does not need to be washed off for the next feeding | Applied to the mother’s nipple. Mothers with a history of wool allergy should not use lanolin before a skin test can be done. |
erythromycin ophthalmic ointment or drops (Ilotycin) | Ophthalmic antibiotic agent | Irritation of eye that lasts 24 to 48 hr Vision may be blurred temporarily | Apply to conjunctival sacs of baby. Wear gloves. Cleanse eye first, if necessary. Spread the ointment from the inner canthus to the outer canthus on lower lid. Do not touch the tube to the eye. After 1 min, wipe off excess ointment. Observe eyes for irritation. |
benzocaine (Dermaplast spray or ointment) | Local anesthetic that inhibits conduction of nerve impulses from sensory nerves, temporarily reducing perception of local discomfort | Urticaria, edema, contact dermatitis | Cleanse area with clear, warm water after each trip to the toilet. Hold spray 6-12 inches from affected area and spray liberally. Use up to four times a day. |
NOTE: Hepatitis B vaccine is no longer given at birth while the patient is still in the hospital but in the physician’s office, as determined by the health care provider. IgG, Immunoglobulin G; IM, intramuscularly. | |||

FIGURE 27-4 Suggested guidelines for assessment of lochia volume. The pad may also be weighed and compared with the weight of a clean dry pad (1 g of weight equals 1 mL). A, Scant, less than 1 inch (2.5 cm). B, Light, less than 4 inches (10 cm). C, Moderate, less than 6 inches (15 cm). D, Heavy, pad saturated within 1 hour.
(From Lowdermilk DL, Perry SE: Maternity and women’s health care, ed 9, St. Louis, 2007, Mosby.)
in postpartum assessments. Hemorrhoids (varicosities of the rectum) usually disappear quickly after delivery if there is no longstanding history of this problem. Use topical anesthetics to relieve pain if ordered by the physician. Sitz baths also provide relief and should be offered if the physician has ordered them. Suppositories may be ordered for hemorrhoid treatment.
Examine the patient’s legs by stretching and straightening each leg, then using dorsiflexion on the foot. Pain in the calf is a positive Homans’ sign, which indicates inflammation of the blood vessels of the leg and possible thrombophlebitis. Notify the physician promptly. Some facilities have policies that restrict the dorsiflexion of the foot out of concern that it may result in a clot being released. In this case, the lower extremities should be closely examined for warmth and redness. Note that early ambulation is the leading means of prevention of this potential complication.
The postpartum assessment can be organized as a head-to-toe assessment with the eight letters BUBBLE-HE (Box 27-9).
Lactation and breastfeeding.
All new mothers should be encouraged to wear a bra regardless of breast size. The bra should be comfortable and fitted to provide support. Encourage breastfeeding mothers to use bras large enough to accommodate the growth that occurs with lactation. Nonnursing mothers need
Box 27-9 Postpartum Assessment: BUBBLE-HE
- Breast: For assessment of the breast, have the patient lie down and remove her bra. Palpate both breasts for engorgement or nodules. Inspect nipples for pressure, soreness, cracks, or fissures.
- Uterus: The top of the uterus, the fundus, should remain very firm. If it becomes soft, the uterine muscles probably are not contracting properly or the uterus has retained placental fragments. Both conditions predispose the patient to hemorrhage. Gently massage the uterus to help the muscles contract and expel placental fragments.
- Bladder: The new mother may urinate frequently the first few days after giving birth. Be alert for signs and symptoms of infection. Also note any dysuria or urinary retention.
- Bowel: Because of early discharge from the hospital, many women leave without having had a bowel movement. Assess for bowel sounds, encourage activity with rest periods, and encourage adequate fluid intake.
- Lochia: Lochia has a definite fleshy scent, but if it has a fetid odor, it may indicate infection. Assess carefully.
- Episiotomy: Most new mothers have an episiotomy and, in some cases, a laceration. (NOTE: There is a move away from doing an episiotomy on the side—either left or right—and possibly even away from doing episiotomies at all, but midline is the site of choice. For a lateral episiotomy, use the following procedures.) Position the patient on her affected side. Instruct her to flex her top leg at the knee and draw it up toward her waist. Use a flashlight and wear gloves. Stand behind the patient and gently lift her top buttock to expose the perineum. Also assess for hemorrhoids.
- Homans’ sign: For patient assessment, position the legs flat on the bed while she reclines in the supine position. Dorsiflex her foot toward the ankle. Assess both extremities. If she reports calf pain, Homans sign is positive; further assessment is needed because a blood clot in a vessel in the leg is indicated.
- Emotional status: Consider the three phases most new mothers pass through:
- 1.The first is “taking in,” the time immediately after birth. She sleeps, depends on others for nurturing and food, and relives the events surrounding the birth.
- 2.Over the next few days, she is “taking hold.” She is preoccupied with the present and concerned about her health and her baby’s condition. She cares for herself and wants to learn to care for her newborn.
- 3.The next phase, “letting go,” comes later in the postpartum period. She reestablishes relationships with other people.
- Monitor the patient’s emotional status, noting how she interacts with her family, her level of independence, sleep and rest patterns, mood swings, irritability, or crying.
Modified from Ferguson H: Planning letter-perfect postpartum care. Nursing 17(5);50, 1987.
a bra that provides adequate compression to inhibit lactation without being uncomfortable.
With the bra removed, inspect and palpate the breasts. Observe for erythema, heat, edema, and engorgement.
Engorgement is an uncomfortable fullness of the breasts that occurs when the milk supply initially comes in. It is a result of venous and lymphatic stasis that occurs during lactation. Filling of the breast with milk usually begins in the axillary region, so palpate both the body and the tail of the breast. Engorgement is usually observed about the third day postpartum and resolves in about 48 hours. Because most patients are home by the time engorgement occurs, teach the new mother the symptoms of engorgement and methods of obtaining relief. If the patient is breastfeeding, interventions such as manual expression of milk and application of warm, moist heat are most useful. If the patient is not breastfeeding, compression of the breasts with a firm bra, wrapped ice packs, and analgesics are most often recommended.
Inspect the nipples for inflammation, fissures, or tenderness. The nipples generally do not cause problems for nonlactating mothers; however, if the patient is breastfeeding, the nipples should be kept soft and supple. Most physicians recommend avoiding soap or other chemicals because they dry the skin and may be ingested by the infant. Plain water and air drying may prevent problems. Some physicians recommend allowing the nipples to dry after feeding without removing the milk residue. If additional moisturizer is needed, small amounts of unscented lanolin or a nipple cream may be used to soften and soothe dry, tender nipples. Modifications in the positioning of the baby may be needed if tender or cracked nipples continue to be a problem.
In addition to assessing the breasts, help the breastfeeding mother succeed in establishing lactation. To establish the lactation response, the breast must be adequately stimulated so prolactin can be released by the anterior pituitary. Once the milk supply is established, prolactin production decreases, and oxytocin, released as the baby suckles, primarily maintains the supply of milk.
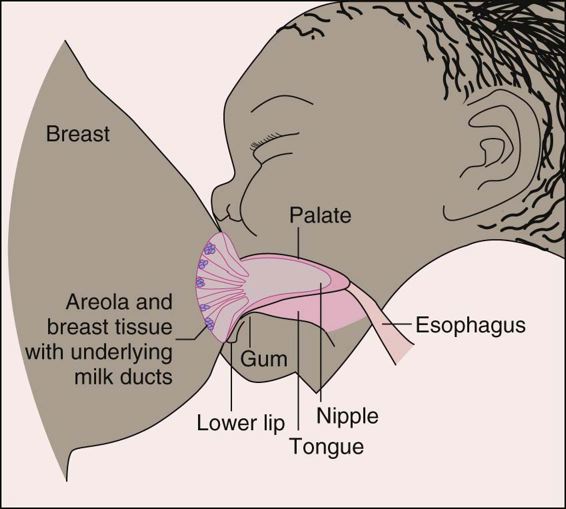
The mother may feel a tingling or prickling sensation, known as the let-down reflex, when feeding time approaches. If the mother nurses the baby at regular, frequent intervals and empties the breasts, the supply of milk increases in response to the baby’s demands. If the breast is not adequately stimulated, the lactation response may not be established. This can happen when the baby has a weak suck or is not put to breast often enough. If the breast is not emptied adequately, the pressure of the milk in the alveoli can also suppress milk production. Incorrect placement at the breast may also lead to problems. If the baby’s mouth grasps only the nipple and does not apply pressure on the lactiferous glands (mammary glands or Montgomery’s glands, consisting of 20 to 24 glands in the areolae of the nipples), milk is not released and the needed stimulation does not occur. This also may lead to nipple trauma and soreness.
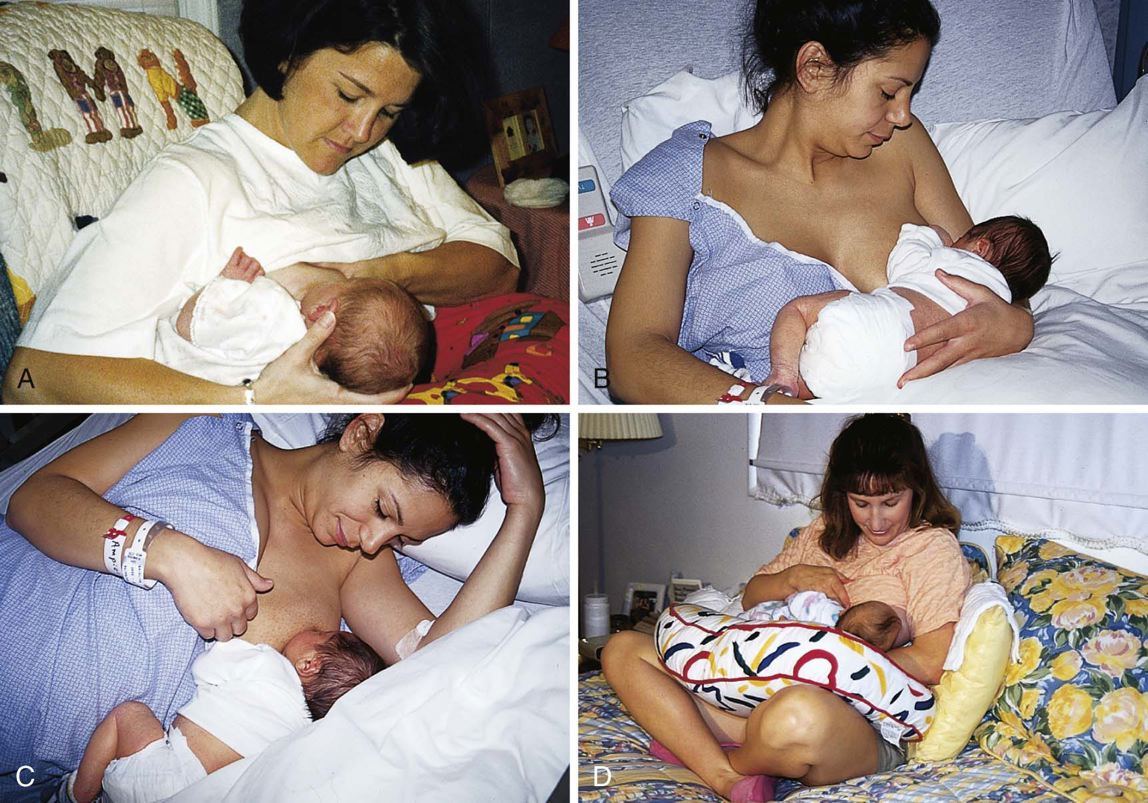
FIGURE 27-5 Positioning the baby for breastfeeding. A, Football hold. B, Cradling. C, Lying down. D, Across the lap.
(B, C, D, Courtesy Marjorie Pyle, RNC, LifeCircle, Costa Mesa, Calif.)
Become knowledgeable about correct breastfeeding techniques so you can instruct the breastfeeding mother. These techniques include correct position and placement of the nipple and areola in the baby’s mouth, stimulation of the infant to enable correct latch-on (attachment of the infant to the breast for feeding), frequency and length of nursing, and care of the breasts. Also assist the mother’s efforts by providing support and encouragement. Lactation consultants, teaching videos, and support groups such as La Leche League are excellent resources that supplement and reinforce teaching by the nurse (Figures 27-5 and 27-6).
Manual pumping of the breasts may be necessary in some cases. The mother whose infant is unable to suckle at the breast at birth may pump to establish lactation and provide milk that can be fed to her baby by alternate means. The mother who must spend an extended time away from her infant, such as while at work, may pump to maintain lactation and provide breast milk for her baby during her absence.
Breastfeeding has many benefits for the mother (Box 27-10). The release of oxytocin during breastfeeding stimulates contraction of the uterus, so it under goes more rapid involution. A lower incidence of breast cancer is found in women who have nursed for at least 3 months. Also, many women who breastfeed report a special closeness to their infants because they provide important nourishment. Human milk provides many factors that are uniquely suited to the infant and enhance growth and development. Human milk has antibacterial and antiviral properties, immunoglobulin, and antiallergy factors that protect the
Box 27-10 Advantages of Breastfeeding
- Antiinfective properties: Immunoglobulins, lymphocytes, and other immune components that are present in breast milk protect the infant against infection. The bifidus factor in breast milk encourages growth of normal bacterial flora in the infant’s gastrointestinal tract.
- • Nutrition: Breast milk is specifically made for the human infant. Its protein, carbohydrate, and fat ratios are thought to be ideal for growth and development. It is well digested and readily absorbed.
- • Growth and development: Breastfeeding promotes better tooth and jaw alignment. It may be less likely to produce obesity in the child, and it may favor optimal bonding between mother and infant.
- • Allergy: Breastfeeding may reduce the incidence of allergies in infants at high risk for allergic conditions.
- • Maternal benefits: Hormones produced in breastfeeding help contract and shrink the uterus. Breastfeeding requires no formula preparation or bottle sterilization and is more economical than formula feeding.
infant against many infections and diseases. Mother’s milk also contains growth factors, digestive enzymes, and proteins that foster the maturation process begun in utero.
Nursing diagnoses and interventions for the breastfeeding patient include but are not limited to the following:
Nursing Diagnosis | Nursing Interventions |
Imbalanced nutrition: less than body requirements, related to nutritional demands during lactation | Review dietary choices |
Instruct patient to continue diet recommended during pregnancy | |
Arrange consultation with a dietitian | |
Inform patient of Women, Infants, and Children (WIC) supplemental food program | |
Anxiety, related to initiating feedings as a result of inexperience | Evaluate patient’s readiness to initiate feedings |
Initiate feedings as soon as possible | |
Position mother and infant for comfort | |
Initiate correct latch-on and position correctly | |
Support and encourage mother in breastfeeding attempts |
Bottle feeding is another choice for the new mother. If the mother chooses not to breastfeed, lactation must be suppressed. This can be accomplished by mechanical means, starting before milk production begins. The woman wears a supportive bra within 4 to 6 hours after delivery. Ice to the breasts also decreases the discomfort that may result from engorgement. She should avoid any form of breast stimulation, such as pumping the breasts, and avoid applying heat to the breasts, such as facing the hot water when showering. Do not restrict maternal fluid intake.