Stages of Labor
June 29, 2023
First Stage: Dilation
The first stage begins with the onset of regular contractions and ends with complete dilation of the cervix (Figure 26-15). This stage is generally the longest stage of labor; it averages 10 to 12 hours in nulliparas and 6 to 8 hours in multiparas. This stage is often divided into the following three phases:
- 1.Latent phase (0 to 3 cm dilation): Contractions occur 5 to 8 minutes apart and last 20 to 35 seconds. Dilation at this point is about the size of a penny. The woman generally is alert and talkative. The nulliparous woman may feel anxious about childbirth. This phase is ideal for teaching and establishing rapport. The nurse or a significant other may be the coach, reviewing techniques learned in prenatal classes. Pain tends to be mild and easily controlled. Backache
- is common. Many women, particularly multiparas, prefer to remain home during this stage. If the bag of waters has not ruptured, many women walk during this stage. Women should be advised that if the membranes rupture, they should seek care to be evaluated.
- 2.Active phase (4 to 7 cm dilation): Contractions occur at 3- to 5-minute intervals and last 40 to 60 seconds. The woman becomes less talkative and focuses on breathing techniques learned during prenatal classes. If she has not already learned breathing techniques, teach them to her during labor. The intensity of the pain increases but still may be manageable without medication.
- 3.Transitional phase (8 to 10 cm dilation): Contractions occur at 2- to 3-minute intervals and last up to 90 seconds. The woman is deeply focused and may not wish to communicate with the nurse or significant other. She may be easily irritated by distractions. If the woman has not requested pain medication earlier, she may desire it at this time. Nausea is common.
Second Stage: Delivery of the Fetus
The second stage of labor begins with complete dilation at 10 cm and ends with the birth of the baby. This stage lasts an average of 30 minutes to 2 hours in nulliparas and 20 minutes to 90 minutes in multiparas. Contractions continue to last 80 to 90 seconds or slightly less.
Once the cervix is completely dilated, the woman usually feels the urge to push and is anxious to do so. Pushing is hard work, and the woman needs ongoing encouragement from the coach and the nurse. Resting between contractions, if possible, is important to conserve energy.
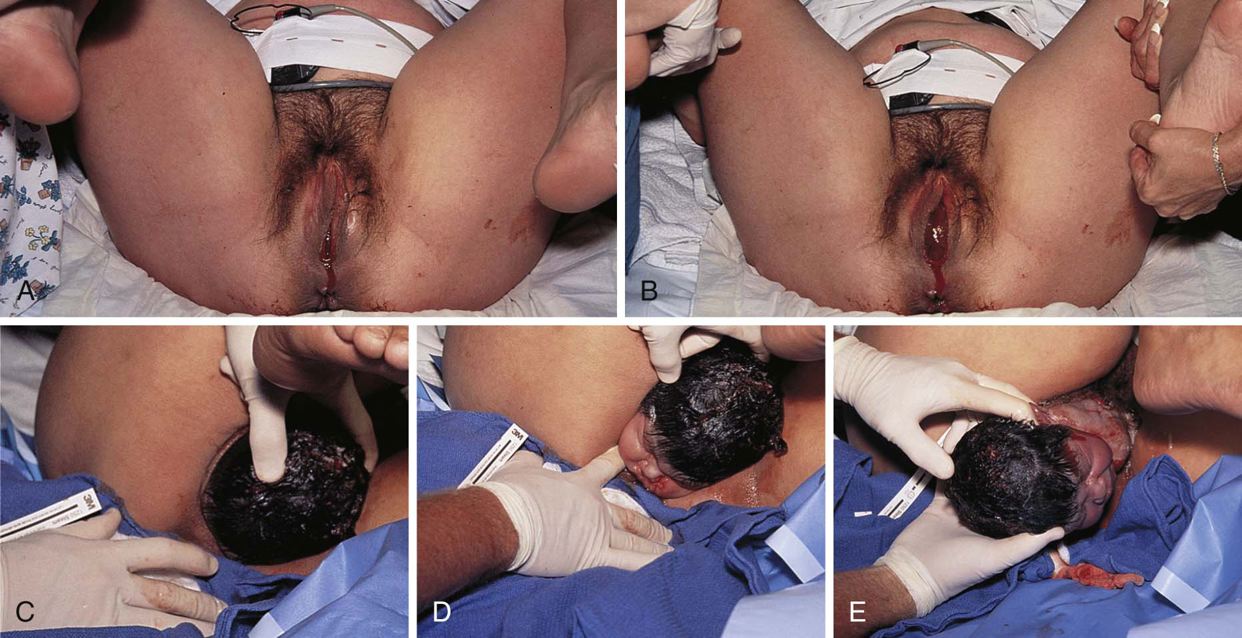
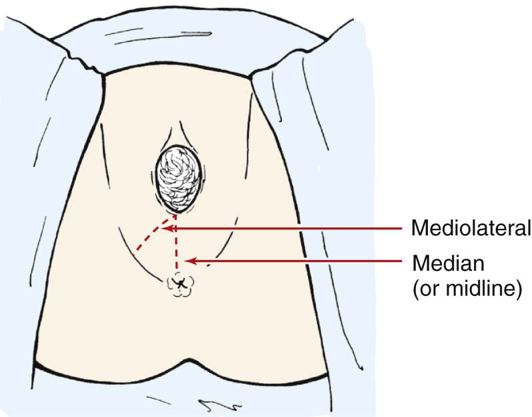
During this stage, the primary care practitioner may provide anesthesia and perform an episiotomy. The episiotomy is a surgical incision of the perineum performed at the end of the second stage of labor (Figure 26-16). Episiotomies were once considered almost standard in vaginal births. Historically, the procedure was performed to reduce bleeding, minimalize tearing, and aid in the prevention of future bowel and bladder complications (Boyles, 2002). In the 1980s, most women with vaginal births had episiotomies. By the mid-1990s, the rate for the procedure was around 30%. In 2005, the number had significantly fallen to an estimated 10% to 25%. Critics of episiotomies report that they are warranted in only about 10% of women birthing vaginally (Hyer, 2009). The most common type of episiotomy is a midline, or median, incision that separates the tissues of the perineum at an anatomic junction. Advantages of the midline episiotomy include ease in completing the procedure, speed of healing, and comfort over the mediolateral incision. Unfortunately, this type does have a greater risk for further extension and tearing. If the perineum is too small or the fetus is anticipated to be large, a mediolateral incision, which involves cutting the muscle, is performed. This is generally more uncomfortable and is done only when necessary. Complications of an episiotomy include infection, blood loss, pain, and painful sexual intercourse.
Immediately after delivery, the baby’s airway is established (see Response of the Newborn to Birth) and the umbilical cord is clamped with two clamps and then severed between the clamps. If there are no complications, show the baby to the parents. Then, either give the infant to the mother to hold or position the infant in a warming unit that allows for close observation and care. If any problems occur with the infant, administer care immediately. This emergency care may need to be performed in the delivery area. Remain calm and supportive to the parents. Be aware that the parents may be alarmed and need support and explanations to allay their fears for the newborn.



Third Stage: Delivery of the Placenta
The third stage begins with the delivery of the infant and ends with the delivery of the placenta. The average for both primiparas and multiparas is 5 to 20 minutes.
When the placenta detaches from the uterine wall, blood suddenly pours out of the vagina. The cord protruding from the vagina lengthens, and the uterus becomes more rounded and firm. The woman may again experience contractions. The size and consistency of the placenta usually permit delivery with one or two pushes. During this time, the primary care practitioner repairs the episiotomy if one was performed. Total blood loss is normally 200 to 300 mL; more than 500 mL of blood lost during delivery is considered excessive. An oxytocic medication, such as oxytocin (Pitocin) or methylergonovine maleate (Methergine), is commonly administered during this stage (Table 26-3). An oxytocic (oxytocin is a hormone produced by the pituitary gland) is a drug that stimulates uterine contractions and works to prevent postdelivery hemorrhage. These medications cause the uterus to contract firmly, compressing blood vessels inside the uterus and keeping blood loss to a minimum.
Fourth Stage: Stabilization
The time immediately after delivery is critical as the mother’s body attempts to recover from the efforts of labor. Usually the mother is monitored closely for 2 to 4 hours after delivery in the birthing room or in a recovery room. Some women, particularly those who had a long or difficult labor and delivery, are exhausted and wish only to rest. Others seem euphoric and wish to talk about the experience or spend time with the baby and their significant other.
Monitor physiologic changes closely during the fourth stage. Assess vital signs, uterine tone, vaginal drainage, and the perineal tissue. During the first hour, perform assessments every 15 minutes. If observations are within normal limits, assessments are done every 30 minutes for the next hour. If all observations remain normal, the woman is transferred to a patient room for
Table 26-3 Medications for Normal Labor and Delivery
GENERIC NAME (BRAND NAME) | ACTION | SIDE EFFECTS | NURSING IMPLICATIONS |
butorphanol (Stadol) | Synthetic, centrally acting analgesic; provides relief of moderate to severe pain during labor | Drowsiness, sedation, headache, vertigo, dizziness, weakness, confusion, insomnia, nervousness, respiratory depression, change in blood pressure, palpitations, bradycardia, nausea, clammy skin, tingling, flushing and warmth, diaphoresis, skin rash, pruritus, increased urinary output Neonatal: respiratory depression, disorganized infant behavior, tendency for frequent crying | Monitor for respiratory depression; do not give if respiratory rate is <15 breaths/min; monitor vital signs; observe neonate for respiratory depression; observe safety precautions because of sedation and dizziness. |
misoprostol (synthetic prostaglandin E; Cytotec) | Used most widely to prevent nonsteroidal antiinflammatory drug–induced gastric ulcer in patients at high risk | Headache, nausea, dyspepsia, vomiting, constipation, flatulence | Some physicians use it to induce labor, especially in the event of fetal death, administered vaginally in the posterior fornix. It is easier on the mother because labor and delivery can be over in as little as 45 min. To induce labor when fetal death has not occurred, administered vaginally into the posterior fornix. |
magnesium sulfate | Decreases acetylcholine in motor nerve terminals, which is responsible for seizure prevention in preeclampsia and eclampsia | Diarrhea; side effects are related to magnesium levels: with >3 mg/dL, depressed central nervous system, blocked neuromuscular transmission that leads to anticonvulsant effects; with >5 mg/dL, depressed deep tendon reflexes; with >12.5 mg/dL, respiratory paralysis | Obtain vital signs q 15 min after IV dose; do not exceed 150 mg/min; monitor cardiac function; time contractions and monitor fetal heart rate; monitor intake and output (should remain ≥30 mL/hr). |
meperidine (Demerol) | Synthetic morphine-like compound that produces comparable analgesic effects and provides relief of moderate to severe pain | Pruritus, dizziness, sedation, weakness, euphoria, respiratory depression, hypotension, palpitations, bradycardia or tachycardia, dry mouth, nausea, constipation, oliguria, urinary retention Neonatal: respiratory depression | It is used less and less frequently. Monitor vital signs closely, especially respiratory rate, depth, and rhythm; encourage deep breathing and coughing to overcome respiratory depressant effects; assess patient’s need for medication as needed; give IM or IV as ordered in smallest effective dose. |
methylergonovine maleate (Methergine) | Stimulates uterine contraction, decreases bleeding | Headache, dizziness, nausea, vomiting, chest pain, palpitations, hypertension, tinnitus, sweating, rash | Monitor blood pressure, pulse, character, and amount of vaginal bleeding; monitor respiratory rate; give IM in deep muscle mass and IV only in emergency. |
oxytocin (Pitocin, Syntocinon) | Acts directly on myofibrils, producing uterine contractions; stimulates milk ejection by breasts | Anaphylaxis, postpartum hemorrhage, cardiac arrhythmias, nausea, vomiting, premature ventricular contractions, hypertension, convulsions Fetal: bradycardia, arrhythmias, jaundice, hypoxia, intracranial hemorrhage | Monitor intake and output ratio, contractions, fetal heart rate, blood pressure, pulse, and respirations. |
prostaglandin E (dinoprostone [Prepidil, Cervidil]) | Stimulates uterine contractions like those seen in normal labor | Uterine contractile abnormalities, nausea, vomiting, diarrhea, back pain, warm feeling in vagina, fever Fetal: heart rate abnormalities, bradycardia | Use caution to prevent contact with skin; wash thoroughly after administration; bring to room temperature before administering; do not force warming process; have patient remain supine for 15-30 min after insertion. |
ritodrine hydrochloride (Yutopar) | Uterine beta2-adrenergic receptor–stimulating effect, which reduces uterine contractions | Erythema, rash, dyspnea, hyperglycemia, headache, restlessness, anxiety, chills, tremor, nausea, vomiting, diarrhea, constipation, altered maternal and fetal heart rates | It is used less and less frequently. Monitor maternal and fetal heart tones during infusion; watch intensity and length of uterine contractions; monitor fluid intake to prevent overload; monitor blood glucose level in patients with diabetes. |
fentanyl citrate (Sublimaze): epidural | Binds with opiate receptors in the central nervous system, altering both perception of and emotional response to pain through an unknown mechanism | Sedation, euphoria, vertigo, headache, confusion, anxiety, depression, seizures, blood pressure deviations, nausea, vomiting, respiratory depression | It is used occasionally. Monitor circulatory and respiratory status and urinary function. Monitor arterial oxygen saturation. |
carboprost tromethamine (Hemabate) | Produces strong, prompt contractions of uterine smooth muscle; used in postpartum hemorrhage from uterine atony not managed with conventional methods | Headache, anxiety, weakness, arrhythmias, eye pain, nausea, vomiting, uterine rupture, backache, leg cramps, wheezing, fever, chills | It is used only by trained personnel in a hospital setting and may be injected into the uterus. |
promethazine hydrochloride (Phenergan) | Prevents but does not reverse histamine-mediated responses; at high dosage, exhibits local anesthetic effects; used as adjunct to analgesics | Sedation, blood pressure deviations, blurred vision, nausea, vomiting, urine retention, seizures | It is used most of the time for postoperative cesarean delivery. Inject deep into large muscle mass. Often used as an adjunct to analgesics. It may be mixed with meperidine in the same syringe. |
nalbuphine hydrochloride (Nubain) | Binds with opiate receptors in the central nervous system, altering perception of and emotional response to pain through an unknown mechanism | Headache, sedation, vertigo, syncope, restlessness, crying, confusion, blood pressure variations, bradycardia, blurred vision, nausea and vomiting, urinary urgency, respiratory depression, asthma Neonatal: disorganized infant behavior, fussiness, refusal to nurse | Usually administer one or two doses and then begin an epidural. Monitor circulatory and respiratory status and bladder and bowel function; withhold dose and notify physician if respirations become shallow or fall below 12 breaths/min. Stool softeners may be ordered. |
hydroxyzine (Vistaril) | Antianxiety antepartum and postpartum adjunctive therapy | Drowsiness, dry mouth, marked discomfort at IM injection site | It is used less frequently. Aspirate IM injection carefully to prevent inadvertent IV injection. Inject deeply into a large muscle mass. Observe for sedation. |
naloxone hydrochloride (Narcan) | Thought to displace previously administered narcotic-opioid analgesics from their receptors (competitive antagonism); indicated for use in known or suspected narcotic-induced respiratory depression in neonates (asphyxia neonatorum) | Tremors, seizures, blood pressure variations, nausea, vomiting Can cause seizure when used with street drugs (of which the health care worker is sometimes unaware) | It is not used as often as it once was. Respiratory rate increases within 1-2 min. Monitor respiratory depth and rate. Be prepared to provide oxygen, ventilation, and other resuscitation measures. Administer IV into umbilical vein. May be repeated q 2-3 min. |
IM, Intramuscularly, intramuscular; IV, intravenously, intravenous. | |||
Box 26-2 Changes in Fetal Heart Rate
Normal Baseline Rate
- • 120 to 160 bpm
Tachycardia
- • Moderate increase to 160 to 180 bpm
- • Marked increase greater than 180 bpm; significant if variability is absent and late or variable decelerations (decreases in the speed or velocity of an object or reaction) are present
Nursing Interventions*
- • Interventions depend on the cause.
- • Reduce maternal fever with antipyretics as ordered and cooling measures.
- • Oxygen at 8 to 10 L/min per face mask may be of some value.
- • Carry out health care provider’s orders to alleviate cause.
Bradycardia
- • Moderate decrease to 100 to 120 bpm
- • Marked decrease to fewer than 100 bpm; significant if variability is decreased or absent or if late or variable decelerations are present
Nursing Interventions*
- • Interventions depend on the cause.
- • Intervention is not warranted in fetus with heart block diagnosed with electrocardiogram.
- • Oxygen at 8 to 10 L/min per face mask may be of some value.
- • Carry out health care provider’s orders to alleviate cause.
- • Scalp stimulation may be performed to determine whether the fetus is able to compensate physiologically for stress (fetal heart rate [FHR] accelerates).
Variability
- • Measures the normal fluctuation of the FHR from the baseline
- • Absent or minimal variability possibly indicative of fetal distress
- • Variability classified as long-term variability (LTV) or short-term variability (STV)
Decelerations
- • Periodic decreases in the FHR in response to contractions; classified as early, late, or variable (Figure 26-17)
- • Early decelerations: caused by pressure on fetal skull; tend to be uniform; onset, shape, and recovery correspond to contractions
- • Late decelerations: caused by decreased oxygen and blood flow to fetus through the placenta; noted at or after the peak of the contraction; may indicate fetal distress, particularly if associated with changes in baseline FHR and absence of variability
- • Variable decelerations: caused by compression on the umbilical cord; occur randomly and onset may be sudden; FHR decreases below normal range
Nursing Interventions*
- • Notify the primary caregiver immediately and initiate appropriate treatment when patient has a prolonged deceleration.
* See Box 26-3 for care of the woman being monitored electronically for fetal status during labor.
the remainder of her hospitalization (unless she is in a birthing center or in a facility that has an LDRP room configuration where she may remain until discharge).
Monitoring Fetal Status
The process of labor is stressful to the fetus, and continuous monitoring of the fetus is important during this time. Fetal heart rate (FHR) is a good indicator of the fetus’s condition. The normal FHR range is 120 to 160 bpm. An increase or decrease of 30 bpm may indicate fetal distress and should be reported immediately (Box 26-2).
Auscultate the FHR, with a fetoscope or a Doppler instrument, every 15 to 30 minutes during the first stage of labor and every 5 minutes during the second stage. Also assess the FHR immediately after rupture of the membranes, particularly if the head is not engaged (i.e., not firmly settled into the pelvis).
Electronic Fetal Monitoring
Frequently, continuous electronic monitors, either internal or external, are applied for electronic fetal monitoring (EFM). Monitors can detect subtle changes of condition before they can be recognized with auscultation. The external, or indirect, mode uses external transducers on the maternal abdominal wall to assess FHR and uterine activity. An ultrasound transducer uses high-frequency sound waves to reflect movement of the fetal heart ventricles. A tocotransducer monitors uterine activity and records frequency and duration of contractions. A strip chart prints out both FHR (upper part of the strip) and uterine activity (lower part of the strip) (Figure 26-18, A). External monitoring can be used in both the antepartal and the intrapartal periods. It does not require rupture of membranes or cervical dilation; however, the tocotransducer cannot assess the intensity of contractions. Maternal position can affect the accuracy of the recordings.
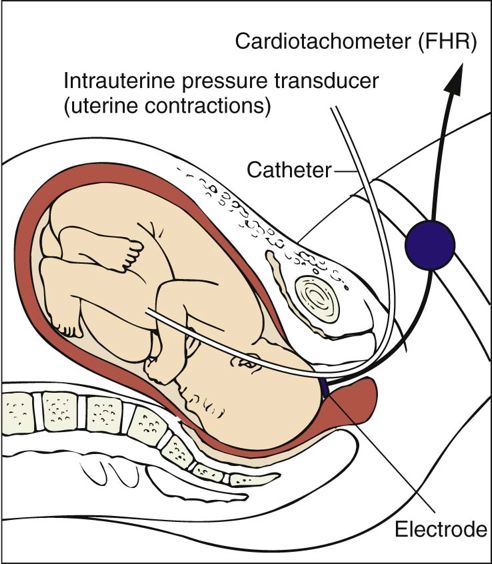
Internal monitoring uses a spiral electrode applied to the presenting part to monitor the FHR (Figure 26-19). An intrauterine catheter is used to monitor frequency, duration, intensity, and resting tone of uterine contractions. This catheter is compressed during contractions, which places pressure on a strain gauge or pressure transducer. FHR and uterine pressure are reflected on a strip chart (Figure 26-18, B). Internal monitoring can be used only during the intrapartal period because membranes must be ruptured and the cervix dilated 2 to 3 cm. Display of FHR and uterine activity is accurate regardless of maternal position. Box 26-3 lists guidelines for care of the woman being monitored electronically for fetal status during labor.
FHR is monitored in relation to the contractions. A decrease in FHR occurs in response to the contractions and is called a deceleration. Decelerations can be early, late, or variable (Figure 26-20 and see Box 26-2). In the United States today, electronic monitoring is routinely used for low-risk, and high-risk, labors.


Fetal Distress
Fetal distress from hypoxia (insufficient availability of oxygen to meet metabolic needs) is indicated with nonreassuring FHR patterns. These patterns can include a progressive increase or decrease in the baseline FHR, progressive decrease in baseline variability, tachycardia (more than 160 bpm), severe bradycardia (less than 100 bpm), persistent late decelerations, and severe variable decelerations with slow return to baseline.



Box 26-3 Care of the Woman With Electronic Fetal Monitoring
The following guidelines relate to patient teaching and the functioning of the monitor.
- •Explain that fetal status can be continuously assessed with electronic fetal monitoring (EFM), even during contractions.
- •Explain that the lower tracing on the monitor strip paper shows uterine activity; the upper tracing shows the fetal heart rate (FHR).
- •Reassure woman and partner that prepared childbirth techniques can be implemented without difficulty.
- •Explain that during external monitoring effleurage can be performed on sides of abdomen or upper portion of thighs.
- •Explain that breathing patterns based on the time and the intensity of contractions can be enhanced by the observation of uterine activity on the monitor strip paper, which shows the onset of contractions.
- •Note peak of contraction; knowledge that a contraction will not get stronger and is half over usually is helpful.
- •Note diminishing intensity.
- •Coordinate with appropriate breathing and relaxation techniques.
- •Reassure woman and partner that the use of internal monitoring does not restrict movement, although she is confined to bed.*
- •Explain that use of external monitoring usually requires the woman’s cooperation during positioning and movement.
- •Reassure woman and partner that use of monitoring does not imply fetal jeopardy.
- •Reassure woman that the equipment is removed periodically to permit the applicator site to be washed and other care to be given.
External Monitoring
Ultrasound Transducer
Function
Monitors FHR with high-frequency sound waves.
Nursing Care
- • Tap transducer before use to ensure sound transmission.
- • Apply ultrasound transmission gel to transducer, clean abdomen and transducer, and reapply gel every 2 hours and as needed.
- • Massage reddened skin areas gently and reposition belt or adhesive device every 2 hours and as needed.
- • Auscultate FHR with stethoscope or fetoscope if in doubt as to validity or tracing.
- • Position and reposition transducer as needed to ensure receipt of clean, interpretable FHR data.
Tocotransducer
Function
Monitors uterine activity via a pressure-sensing device placed on the maternal abdomen.
Nursing Care
- • Position and reposition every 2 hours and as needed on the fundus, the area of least maternal tissue.
- • Keep abdominal strap snug but comfortable for the laboring woman.
- • Adjust pen-set between contractions to print between 10 and 20 mm Hg on the monitor strip paper.
- • Palpate fundus every 30 to 60 minutes to assess strength of contraction; only frequency and duration of contractions can be assessed with tocotransducer.
- • Do not determine woman’s need for analgesia based on uterine activity displayed on monitor strip.
- • Gently massage reddened areas under transducer and belt every hour and as needed.
Internal Monitoring
Spiral Electrode
Function
Obtains fetal electrocardiogram from presenting part and converts it into FHR.
Nursing Care
- Ensure that wires are appropriately attached to leg plate.
- • Reapply electrode paste to leg plate if needed.
- • Observe FHR tracing on monitor strip for variability.
- • Turn electrode counterclockwise to remove; never pull straight out from presenting part.
- • Administer perineal care after the woman voids during labor and as needed.
Intrauterine Catheter
Function
Catheter (solid or fluid-filled) that monitors intra-amniotic pressure internally.
Nursing Care
- • Flush open system catheter with sterile water before insertion and as needed.
- • Ensure that the length line on catheter is visible at introitus.
- • For closed-system catheters, turn off stopcock to woman; then, with pressure valve of strain gauge released, flush strain gauge, remove syringe, and set stylus to 0 line of chart paper; test further according to manufacturer’s instructions every 3 to 4 hours and as needed.
- • Check proper functioning by tapping catheter, asking woman to cough, or applying fundal pressure; observe appropriate inflection on strip chart.
- • Keep catheter taped to woman’s leg to prevent dislodgment.
* Portable telemetry monitors allow the FHR and uterine contraction patterns to be observed on centrally located electronic display stations. These portable units permit ambulation during electronic monitoring.
Another indication of fetal distress is greenish-stained amniotic fluid in a cephalic presentation. The color is a result of meconium (the infant’s first stool, a viscid, sticky; dark greenish brown, almost black; sterile, odorless stool) being released from the fetal rectum in response to hypoxia (which increases intestinal activity and relaxes the anal sphincter). This color is often referred to as meconium staining. Table 26-4 describes characteristics of amniotic fluid.
Nurses who care for women during childbirth are legally responsible for correctly interpreting the FHR pattern, indicating appropriate nursing interventions based on that pattern, and documenting the outcome of those interventions. Notify the primary caregiver in a timely manner if an abnormal FHR pattern is detected. Initiate the institutional chain of command if health care providers disagree on the interpretation of the FHR pattern and the intervention necessitated.
Response of the Newborn to Birth
The process of delivery is stressful to the newborn. Rapid adaptation from the intrauterine climate to that of extrauterine life is essential if the newborn is to survive.
The infant’s physical condition is evaluated at birth. Most facilities use an evaluation guide called the Apgar score (Table 26-5). This scoring is done at 1 and 5 minutes of age. The score can range from 0 to 10, with 8 to 10 considered optimal. The criteria used include heart rate, respiratory effort, muscle tone, reflex irritability, and skin color. A low score indicates serious problems that may necessitate resuscitation. A high score indicates good condition, necessitating only routine care.
In utero, the fetus’s need for oxygen was met by the mother. Once the umbilical cord is severed, the newborn must breathe to obtain oxygen. Fetal lungs
Table 26-4 Assessment of Amniotic Fluid Characteristics
CHARACTERISTIC OF FLUID | NORMAL FINDING | DEVIATION FROM NORMAL FINDING | CAUSE OF DEVIATION FROM NORMAL |
Color | Pale, straw-colored; may contain white flecks of vernix caseosa, lanugo, scalp hair | Greenish brown | Hypoxic episode in fetus results in meconium passage into fluid May be normal finding in breech presentation, related to pressure exerted on fetal abdominal wall during descent |
Yellow-stained fluid | Fetal hypoxia ≥36 hr before rupture of membranes; fetal hemolytic disease; intrauterine infection | ||
Port-wine color | Bleeding associated with premature separation of the placenta (abruptio placentae) | ||
Viscosity and odor | Watery; no strong odor | Thick, cloudy, foul-smelling | Intrauterine infection Large amount of meconium makes fluid thick |
Amount (normally varies with gestational age) | 400 mL (20 wk of gestation) | >2000 mL (32-36 wk of gestation) | Hydramnios (excessive amount of amniotic fluid): associated with congenital anomalies of the fetus when fetus cannot drink or fluid is trapped in the body (e.g., fetal gastrointestinal obstruction or atresias); increased risk with maternal pregestational or gestational diabetes mellitus |
1000 mL (36-38 wk of gestation) | <500 mL (32-36 wk of gestation) | Oligohydramnios (a condition in which the volume of amniotic fluid is <300 mL in the third trimester): associated with incomplete or absent kidney; obstruction of urethra; fetus cannot secrete or excrete urine | |
Adapted from Lowdermilk DL, Perry SE: Maternity and women’s health care, ed 9, St. Louis, 2007, Mosby. | |||
Table 26-5 Apgar Scoring Chart
SIGN | 0 POINTS | 1 POINT | 2 POINTS |
Heart rate | Absent | Slow, <100 bpm | >100 bpm |
Respiratory effort | Absent | Slow, irregular | Good crying |
Muscle tone | Flaccid, limp | Some flexion of extremities | Active motion |
Reflex irritability | No response | Grimace | Vigorous cry, cough, or sneeze |
Color* | Pale blue | Body pink, extremities blue | Completely pink |
* Skin color or its absence may not be a reliable guide in nonwhite infants, although melanin (the pigment that gives color to the skin) is less apparent at birth than later.
Box 26-4 Suctioning With a Bulb Syringe
- • Suction the mouth first to prevent the infant from inhaling pharyngeal secretions by gasping as the nares are touched. This is necessary because the neonate is an obligatory nose breather.
- • Compress the bulb (see figure) and insert it into one side of the mouth. Avoid the center of the infant’s mouth, which could stimulate the gag reflex.
- • Suction the nasal passages one nostril at a time.
- • When the infant’s cry does not sound as though it is through mucus or a bubble, stop suctioning. The bulb syringe should always be kept in the infant’s crib.
- • Give the parents demonstrations on how to use the bulb syringe and ask them to perform a return demonstration.
Bulb syringe. Bulb must be compressed before insertion.
must be mature enough that the alveoli can expand adequately. As the infant lungs begin to mature, they begin to produce increasing amounts of a substance called surfactant, which decreases surface tension within the alveoli and permits inflation. At the time of delivery, a combination of chemical, thermal, tactile, and mechanical changes initiates the first breath.
The airway must be cleared of fluids that are in the lungs. Some fluids are forced from the lungs as the thorax passes through the pelvis during delivery. Use a bulb syringe to remove excess fluid from the mouth and nasopharynx (Box 26-4). Positioning of the infant is also important (Figure 26-21).
Warmth is necessary to prevent a rapid drop in body temperature. The environment in utero is approximately 99° F (37.2° C); the external environment in the delivery room is usually about 70° F (21.1° C). To prevent hypothermia, immediately dry the infant to help reduce heat loss from evaporation. Then, place the baby in contact with the mother’s skin, especially if she wishes to breastfeed, or transfer the baby to a radiant warming unit.
If no complications occur, the infant remains in the mother’s view until her care is completed. Place identification bracelets on both mother and baby before they leave the delivery room. A bracelet is also worn by the baby’s father or other person designated by the mother at many institutions. These are used to verify infant identification and match it with that of the mother until discharge. Footprinting the infant is another method of identification; this may be done in the delivery area or in the nursery. Additional security devices that may be used by a birthing unit include microchips placed in the cord clamp or bracelets.
