The Medical Assistant’s Role in Examination, Diagnostic Procedures, and Treatments
April 11, 2024
The Medical Assistant’s Role in Examination, Diagnostic Procedures, and Treatments
Learning Objective: Examine the medical assistant’s role in examinations, diagnostic procedures, and treatments for conditions of eye and ear.
As a medical assistant, you may be involved in assisting with the examination, diagnostic procedures, and treatments. Having an understanding of what will be required of you during those processes will help you provide the best possible care for your patients and be the best assistant for your provider. The following sections describe your role.
Assisting with the Examination and Diagnostic Procedures of the Eye
Learning Objective: Describe the medical assistant’s role in assisting with examinations and diagnostic procedures of the eye.
In a primary care department, the examination of the eye is a screening examination. If the provider suspects that there may be an issue with a patient’s eyes, the patient will likely be sent to an ophthalmologist for further evaluation and treatment. There are several screening diagnostic procedures that a medical assistant can administer when directed to do so by the provider. The following sections discuss how the medical assistant is involved in the examination and diagnostic procedures of the eye.

FIGURE 16.14 Slit-lamp examination. A high intensity beam of light is projected through a narrow slit and a cross section of the illuminated part of the eye is examined through a magnifying lens. From Leonard, P: Building a medical vocabulary, ed 11, Philadelphia, 2021, Saunders.
Assisting with the Examination of the Eye
A complete examination of the eye is technical and requires expensive equipment and the expertise of an ophthalmologist or optometrist. However, a primary care provider performs some basic examinations and treatments of the eye. The ophthalmoscope is used to examine the interior of the eye. It projects a bright, narrow beam of light through the lens and illuminates the interior parts of the eye and retina. It is helpful for detecting disorders of the eyes and certain systemic disorders, such as capillary changes that occur with diabetes mellitus.
The eyelids are examined for edema, which may be the result of nephrosis, heart failure, allergy, or thyroid deficiency. Blepharoptosis, also called ptosis, is drooping of the upper eyelid that can be caused by a disorder of the third cranial nerve, muscular weakness as seen in muscular dystrophy, or myasthenia gravis.
The pupils of the eyes are normally round and equal. Normal pupils constrict rapidly in response to light. This is demonstrated by shining a bright, pinpoint light into one eye from the side of the patient’s head. The pupil of an illuminated eye constricts, and the pupil of the other eye constricts equally. This test is called light and accommodation (L&A). The eyes of an older patient do not accommodate as well as those of a younger person. Each eye is checked this way. The patient is then asked to look at the provider’s finger as it is moved directly toward the patient’s nose to check for eye coordination. If the pupils are equal and round, respond normally to light, and adjust and focus on objects at different distances in a reasonable length of time, the provider charts the acronym PERRLA (which stands for “pupils, equal, round, reactive to, light [and], accommodation”).
PERRLA
P Pupils
E Equal
R Round
R Reactive to
L Light (and)
A Accommodation
Special techniques used in the ophthalmologist’s office include examinations performed with a slit lamp biomicroscope (Figure 16.14). This device is used to view fine details in the anterior segments of the eye. It may be used to view a foreign body because it gives a well-illuminated and highly magnified view of the area. For this examination, the provider first orders the administration of a mydriatic eye drop to dilate the pupil and enhance the visualization of eye structures.
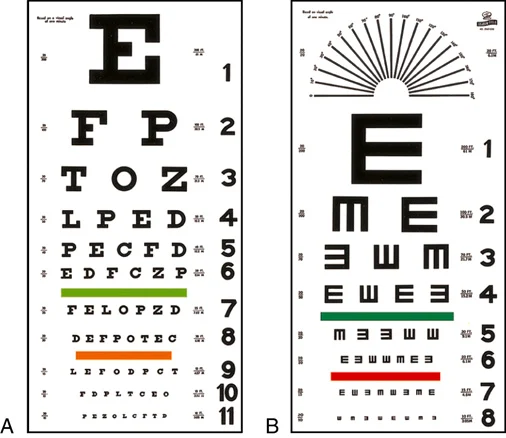
FIGURE 16.15 (A) Snellen visual acuity chart. (B) Tumbling E chart. From Wilson SF, Giddens GF: Health assessment for nursing practice, ed 5 St. Louis, 2013, Elsevier.
A patient with exophthalmia (abnormal protrusion of the eye, possibly resulting from an overactive thyroid or a tumor behind the eyeball) is checked with an exophthalmometer. This instrument measures how far the eye protrudes beyond the edge of the eye socket and helps determine the level of tissue swelling and enlargement behind the eye.
Distance Visual Acuity
Determining distance visual acuity frequently is part of a complete physical examination (see Procedure 16.1). It is widely used in schools and industry and is the best single test available for vision screening. Many cases of myopia, astigmatism, and hyperopia have been detected with this routine test. The chart most commonly used is the Snellen alphabetical chart (Figure 16.15A). This chart displays various letters of the alphabet, which the patient must identify in ever smaller font sizes. Patients with limited knowledge of the English alphabet can be tested with the E chart (Figure 16.15B). In addition, a chart that uses pictures and symbols is available. This chart is used for young children or individuals who do not know the alphabet. To avoid patient confusion over the E chart or the symbol chart, the medical assistant should review the charts with patients first to make sure they know how to demonstrate the E visualized or the meaning of each picture or symbol. The symbol on the top line of the chart can be read at 200 feet by people with normal vision. In each of the succeeding rows, from the top down, the size of the symbols is reduced so that a person with normal vision can see them at distances of 100, 70, 50, 40, 30, and 20 feet consecutively.
The patient must not be allowed to study the chart before taking the test. The room or hall should be long enough that the 20-foot distance can be marked off accurately and without interruptions from patient and staff traffic. The chart should be hung at the patient’s eye level and illuminated with maximum light, without glare on the chart. Most adults do not need the standard Snellen chart explained, but if the E chart is used, an explanation must be given as to how the E’s are to be read. The patient may point up or down or right or left toward the part of the letter that is open. If the E chart is to be used for a child, practice with an index card with a large E drawn on it before the child is tested. Turn the card in different directions to simulate the position of the “fingers” of the E on the chart and give children the opportunity to demonstrate the direction of the E fingers by pointing their own fingers in the same direction (Figure 16.16).
Because this is a gross screening of distance visual acuity, the eyes are typically tested with corrective lenses; therefore, the patient should not remove glasses or contact lenses unless the provider requests it. Indicate in the patient’s health record whether the assessment was done with or without corrective lenses. Record the results of each eye separately and as fractions. The numerator (top number) is the distance of the patient from the chart (always 20 feet), and the denominator (bottom number) is the lowest line read satisfactorily by the patient. For example, if the patient reads the 20 line at 20 feet, the fraction 20/20 is recorded for that eye. The last line the patient can read without squinting or straining and with no more than two mistakes is the line recorded in the patient’s record for that eye. The medical assistant should document the outcomes of the test, specifying the results for each eye and both eyes. The Joint Commission no longer recommends using medical abbreviations for the eyes and ears because they are frequently confused or misinterpreted; therefore, the medical assistant must now document right eye, left eye, and both eyes.
Interpreting Snellen Results
• The patient always stands 20 feet from the chart.
• Each result is a record of how well the patient can see compared with normal vision.
• Example: A patient with a 20/40 reading can see that line correctly standing at 20 feet, but an individual with normal vision can see the same line correctly at 40 feet, so the patient’s vision is not as acute as someone with normal vision.
• Example: A patient with a 20/15 reading can see that line accurately standing at 20 feet, but a person with normal vision must stand at 15 feet to have the same vision, meaning the patient’s vision is better than someone with normal vision.

FIGURE 16.16 Visual acuity test with the E chart.
16.3
Critical Thinking Application
Susie Anthony, a 19-year-old patient, is being seen today for a general eye examination. The provider orders a routine Snellen test, and Kim administers it. Susie wears contacts. With her right eye, she reads without errors to the 20/25 line; however, she squints and makes three errors at the 20/20 line. With her left eye, Susie makes two mistakes at the 20/30 line; with both eyes, she reads the 20/25 without errors. How should Kim document this procedure?
Near Visual Acuity
Near visual acuity can be tested with the near vision acuity chart (Figure 16.17). This test is given to screen for presbyopia or hyperopia. If the patient wears corrective lenses, they should be worn during the test. The size of the type on the card varies from a 66-point font (newspaper headlines) to a 3-point font (medicine bottle labels). The test should be given in a well-lit room, with the patient holding the card approximately 14 to 16 inches away. As with the Snellen examination, the near visual acuity test is given for each eye, starting with the right eye. The eye not being tested should be covered with an occluder but left open. The patient should be monitored for indications of difficulty, such as squinting or tearing. The patient reads the card, starting at the top until reaching the smallest print that can be read. The medical assistant should document the number at which the patient had no more than two errors for each eye and the two eyes together, whether corrective lenses were worn, and any signs of eyestrain.
Ishihara Color Vision Test
Defects in color vision are classified as congenital or acquired. Congenital defects are caused by an inherited color vision defect and are found most often in males. Acquired defects are caused by eye injury or disease. The Ishihara test is a simple, convenient, and accurate procedure that detects total color blindness, in addition to the red-green blindness prevalent in congenital blindness (see Procedure 16.2). The test assesses the perception of primary colors and shades of colors.
The test booklet contains polychromatic plates made of colored dots in numeric patterns. The numbers are one color, and the background dots are a different color. Patients with average visual acuity can read the number within the dot matrix without difficulty. Patients with color vision defects are unable to read the number, or they see a totally different number. A section of plates is included that contains colored line trails through a background of dots. These plates are designed to be used with children and adults who are unable to read numbers. In this situation, the patient uses a finger to follow the dotted trail through the picture.
The test should be administered in a quiet room that is well illuminated by sunlight, not by artificial lighting. If this cannot be done, the best situation possible is created by adjusting lights to resemble the effect of natural daylight. The test uses 14 color plates. The basic test consists of plates 1 through 11. Plates 12 through 14 are used if the patient appears to be having difficulty with red-green differentiation. The medical assistant records the number of plates read correctly. If the score is 10 or higher, the patient is within the average range. If the score is 7 or lower, the patient is suspected of having a color deficiency, and the ophthalmologist performs additional assessment tests using more precise color vision testing equipment.
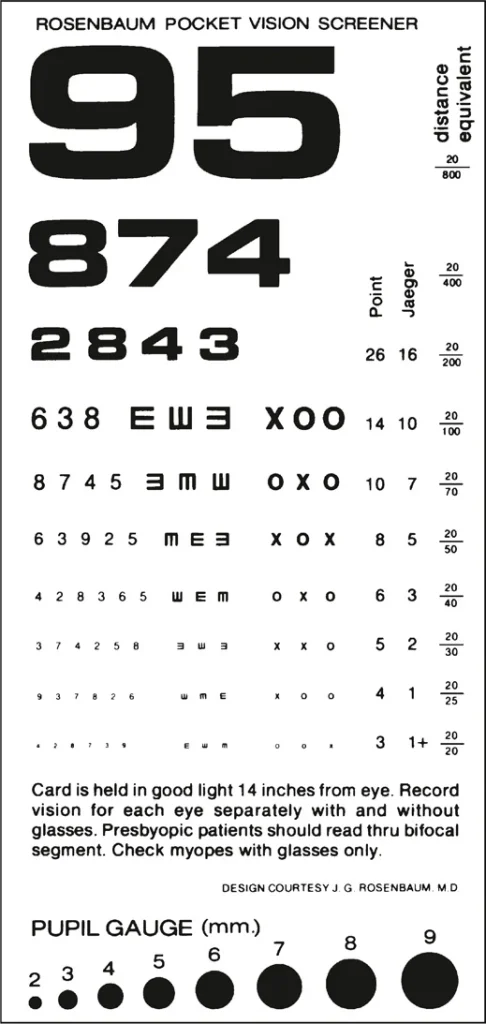
FIGURE 16.17 Near vision acuity chart.
Assisting with Treatments of the Eye
Learning Objective: Describe the medical assistant’s role in treatments of the eye.
Patients with ophthalmology conditions are prescribed a variety of medications. The following are some of the more common classifications of medications used for this specialty:
• Topical antibiotic ointments: Used to treat bacterial infections
• Anti-inflammatory agents: Used to reduce inflammation
• Anti-infectives: Used to treat viral infections
Refer to TABLE 16.2 for information on the classification, including indications for use, desired effect, side effects, adverse reactions, and generic and trade names. Medical assistants should be familiar with medications that are prescribed to patients.
Eye Irrigation
The eye is irrigated to relieve inflammation, remove drainage, dilute chemicals, or wash away foreign bodies. Sterile technique and equipment must be used to prevent contamination (see Procedure 16.3). Follow the procedure as ordered, making sure the patient is comfortable. Record the treatment in the patient’s health record immediately after it has been determined. Remember, if it is not recorded, it has not been done.
Foreign bodies in the eye are very irritating and may cause considerable pain. Most foreign bodies are superficial and can be removed easily. Occasionally, a foreign particle may be deeply embedded, requiring eye surgery. Notify the provider immediately if a patient comes into the office with something in their eye.
The first objective of the provider’s examination is inspection. The patient is asked to look to either side and up and down so that the anterior surface of the eye can be inspected. For the provider to fully inspect under the upper lid, the patient must cooperate by looking downward while the provider everts the upper lid using a cotton-tipped applicator. While the lid is maintained in an everted position, any foreign materials may be rinsed away with sterile water or saline solution. If the provider’s order is for you to remove the foreign body, do so with irrigation only. If this technique is unsuccessful, cover both of the patient’s eyes with a gauze dressing and notify your supervisor immediately. The eyes track each other, so to prevent movement in the affected eye, both eyes must be covered to prevent possible eye trauma.
Safety Alert
Never attempt to remove a foreign body from the cornea using a cotton-tipped applicator. Scratches to the cornea may result, causing scar formation and impaired vision.
Table 16.2
Medication Classifications
| Antivirals | Indications for use: Treat viral infections, including oral and genital herpes, influenza, and HIV. Desired effects: Inhibit the growth or reduce the spread of viral cells. Side effects and adverse reactions: Confusion, diarrhea, headache, kidney disease, urticaria, vomiting. | Oseltamivir (Tamiflu) Acyclovir (Zovirax) |
|---|---|---|
| Mydriatics | • Indications for use: Ophthalmic procedures. • Desired effect: Dilate the pupil; some cause paralysis of the ciliary muscle. • Side effects and adverse reactions: Stinging, burning, dry mouth, urine retention. | • Atropine (Isopto Atropine) • Cyclopentolate (Cyclogyl, Pentolair) |
16.4
Critical Thinking Application
The provider tells Kim to irrigate the left eye of a 22-year-old patient to remove a foreign body. She is to irrigate the eye with normal sterile saline solution until clear. How should Kim document this procedure?