The Medical Assistant’s Role in Examinations, Diagnostic Procedures, and Treatments
April 11, 2024
The Medical Assistant’s Role in Examinations, Diagnostic Procedures, and Treatments
Learning Objective: Examine the medical assistant’s role in examinations, diagnostic procedures, and treatments for neurologic diseases and disorders.
Neurologic diseases are common in primary care and urgent care departments, as well as in neurology and neurosurgery departments. Medical assistants help the provider with the examination, diagnostic procedures, and treatments.
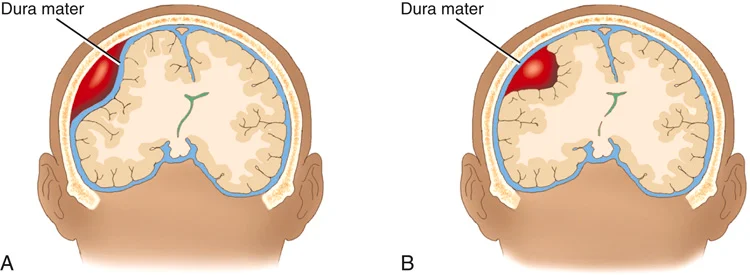
FIGURE 22.15 (A) Epidural hematoma. (B) Subdural hematoma. From Damjanov I: Pathology: a color atlas, St. Louis, 2000, Mosby
Assisting with the Examination
Learning Objective: Describe the medical assistant’s role in examinations for neurologic diseases.
As with other physical examinations, a careful history presents the provider with valuable clues for diagnosing neurologic diseases. Such clues may include a record of seizures, syncope, diplopia (double vision), incontinence, or any previously mentioned subjective symptoms. The patient’s general health often complicates a neurologic diagnosis.
Neurologic Examination
As part of the medical history, the provider may ask a medical assistant to give and score a neurologic status exam (if this is within the medical assistant’s scope of practice for that state and agency). This exam tests the patient’s cognitive functions and provides a baseline of neurologic information for the provider (FIGURE 22.16; also see Procedure 22.1). Part of the exam also requires gathering information from the patient’s caregiver.
The provider will do a neurologic examination, also called a neuro exam, to evaluate the functioning of the patient’s nervous system. During the examination, the provider may determine the effect of the symptoms on the patient’s emotional status, intellectual performance, cognitive ability, and general behavior (see Procedure 22.2). Grooming and mannerisms are carefully observed, as is the patient’s ability to communicate effectively, including the appropriate use of speech, language, and writing skills. The exam may assess many areas:
• Mental status: The patient’s level of awareness of person, place, and time are assessed. “Person” is assessed by asking the person’s name. “Place” is assessed by asking where the patient is. “Time” is assessed with questions related to what year or day it is. If the patient provides the correct answers, providers may document “Alert and oriented,” “Alert and oriented to person, place, and time,” or “A&O×3.”
• Functioning of the cranial nerves: TABLE 22.1 describes how the nerves are assessed.
• Motor function, balance, and coordination: To assess these areas, the patient needs to do the following:
• Push or pull against the provider’s hand with each extremity
• Walk following a line on the floor
• Stand with the eyes closed
• Touch the nose with the eyes closed
The medical assistant’s role in the neuro exam differs among facilities. The medical assistant may need to set up for the exam. Some providers may have the medical assistant remain in the room and assist by handing them supplies and helping the patient change positions. The medical assistant may also be asked to document the provider’s findings during the exam.
Assisting with Diagnostic Procedures
Learning Objective: Describe the medical assistant’s role in diagnostic procedures for neurologic diseases.
The medical assistant helps with diagnostic procedures by scheduling and preparing patients for procedures. If tests require restrictions on food or fluids, the medical assistant should address the following points with the patient after talking with the provider:
• Can the patient have water prior to the test?
• Which medications should the patient take prior to the test, or when can the patient resume the current medications?
TABLE 22.3 describes common diagnostic procedures used for neurologic diseases. The medical assistant may need to screen the patient for specific allergies, medications, and so on prior to the scheduling of the procedure. For some procedures, a signed consent form is required. The patient should be notified of what will be experienced during the procedure and any follow-up care required after the test. The following sections describe the lumbar puncture and the electroencephalography procedures in more detail.
Lumbar Puncture
A lumbar puncture (LP), also known as a spinal tap, is done to collect a small amount of CSF, to measure the pressure of the CSF, and to inject medication into the spinal cord structures. These medications may include spinal anesthetic for surgery, chemotherapy for cancer treatment, and contrast dye (for x-ray procedures, such as myelography). In ambulatory care, the most frequent reason for an LP is to obtain a sample of the CSF. The CSF is analyzed to help confirm or rule out many diseases, including meningitis, encephalitis, cancer, and dementia (TABLE 22.4).
In preparation for the procedure, the patient should be asked if any medication or herbal products have been taken that may increase the risk of bleeding (e.g., anticoagulant and antiplatelet medications, garlic, ginger, St. John’s wort, and ginseng). The patient may be restricted from eating or drinking 3 or more hours prior to the procedure. The provider will explain the procedure to the patient, and a consent form is signed prior to the procedure.
The patient is placed in either a left side-lying position with the knees drawn up to the chest or in a sitting position leaning forward on a stable surface (see Procedure 22.3). For an infant or young child, the medical assistant might need to hold the child in a side-lying position during the procedure.
The site is cleansed with an antiseptic, and a local anesthetic is injected to numb the area. The provider then inserts a hollow needle between the third and fourth or the fourth and fifth lumbar vertebrae and advances it into the subarachnoid space (FIGURE 22.18). The CSF flows out of the needle into the sterile collection tubes. Usually, 1 to 2 mL of fluid is needed in each tube. When multiple tubes are required, a total of 10 to 15 mL of CSF is typically collected. The tubes need to be numbered in the order that they are collected. The needle is removed, and a bandage or small dressing is applied to the site.
After the procedure, the patient typically needs to lie down for about an hour and drink a lot of fluid. If more CSF is removed, the patient may need to lie down for a longer period of time. Prior to leaving the ambulatory care facility, the provider will check the insertion site and assess if the patient has any issues (e.g., problems moving the legs). The patient should not drive and will need to rest at home the for remaining part of the day.
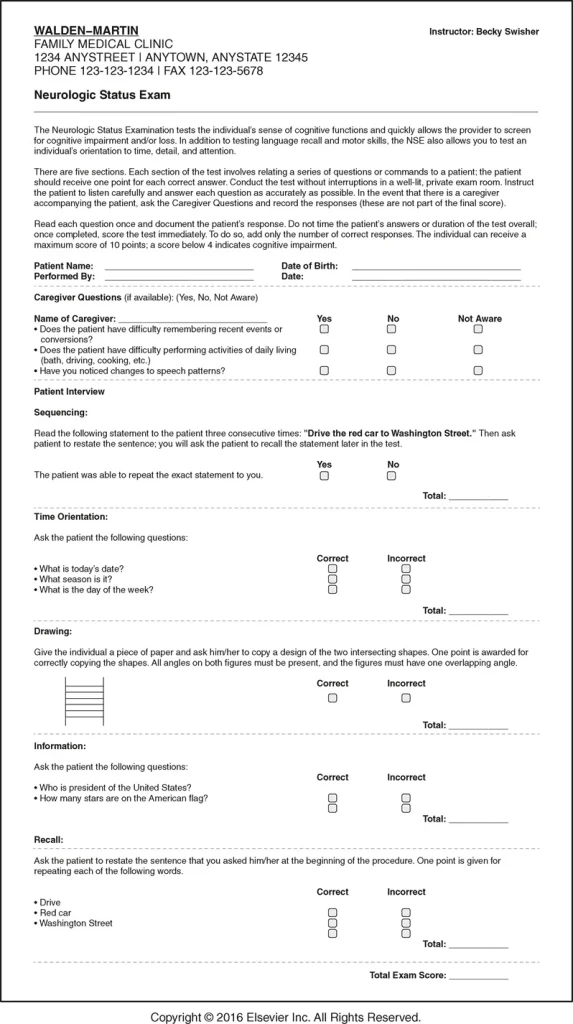
FIGURE 22.16 Neurologic Status Exam Form.
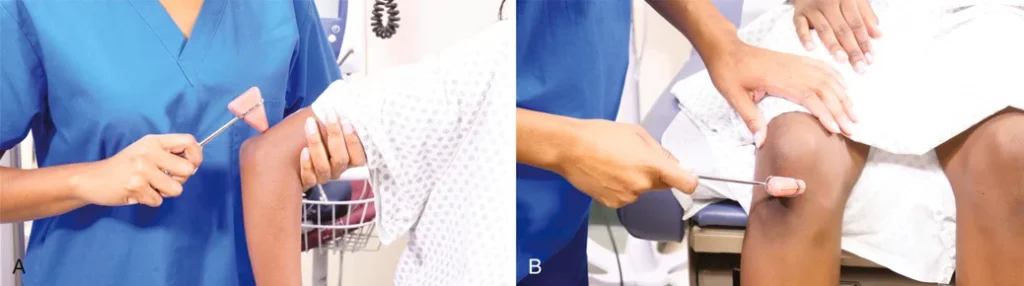
FIGURE 22.17 The provider checks (A) the triceps reflex and (B) the quadriceps reflex.
Table 26.5
Common Abbreviations and Symbols Used in Medication Documentation
| Procedure | Description | Patient Preparation |
|---|---|---|
| Cerebral angiography | Used to see how the blood flows through the brain. A person must lie on the x-ray table without moving. The head is held still. A local anesthetic is given in the groin area, and a catheter is threaded through an artery in the groin until it reaches the neck. X-ray is used to help guide the process. A dye is injected and highlights the blood flow through the brain. | Screen for bleeding problems or taking anticoagulants, allergy to contrast dye, pregnancy, or kidney function problems. The patient may not eat or drink for 4 to 8 hours prior to the test. The patient may feel a brief discomfort during the anesthetic injection and the threading of the catheter. The contrast dye may cause a warming or burning feeling on the face and head. |
| Cerebral spinal fluid analysis | CSF is analyzed to determine any abnormalities. The specimen is gathered by a lumbar puncture (spinal tap) performed by a provider. An anesthetic will be given. A needle is inserted, and the fluid is collected. The CSF is then sent to the laboratory for testing. | Screen for bleeding problems or taking anticoagulants. A consent form must be signed. The patient may be put in an uncomfortable position during the test and will need to hold the position through the procedure. The patient may feel a sting when the anesthetic is injected. |
| Electromyography (EMG) | Used to test the health of nerves and muscles. A fine needle with an electrode is inserted into the muscle. The electrode picks up the electrical activity from the muscle during activity and at rest. The activity is recorded. | Screen if taking an anticoagulant. Patient should avoid using creams and lotions on the day of the test. The patient should have normal body temperature because a lowered temperature can affect the test. The patient may feel the insertion of the needles. After the test, the muscle may be tender. The patient may have bruising for a few days. |
| Nerve conduction velocity (NCV) test | Usually done with EMG. Done to test the speed of electrical signals as they move through a nerve. Electrode patches are placed on the skin over nerves and give off a mild electrical impulse. The electrical activity is recorded by other electrodes. | Screen if the patient has a cardiac defibrillator or pacemaker. Patient should avoid any lotions, sunscreen, perfume, or moisturizer on the test day. The patient may feel the impulse and have some discomfort. |
| Nerve biopsy | The removal of a small piece of the nerve for examination. After applying an analgesic, the provider makes a small surgical incision and removes a piece of the nerve from the ankle, forearm, or rib area. | There is no special preparation. The patient may feel the injection of the local anesthetic medication. The biopsy site will be sore for a few days after the test. |
Lumbar punctures may cause a number of conditions:
• Post-lumbar puncture headaches due to CSF leaking into nearby tissues. The patient may experience nausea, vomiting, and dizziness. Usually, the headaches resolve after lying down. These headaches may last for a week or more after the procedure.
• Bleeding at the site or into the epidural space.
• Brainstem herniation.
• Back discomfort, tenderness, or pain in the lower back. Pain may radiate down the back of the legs.
The patient should notify the provider of any abnormalities, including numbness and tingling in the legs, draining or pain at the injection site, an increase in the number or intensity of headaches, and inability to urinate.
Electroencephalography
Electroencephalography (EEG) is used to record the brain wave activity of a patient. An EEG may be done to rule out or confirm seizure activity, AD, psychosis, and narcolepsy, a sleep disorder.
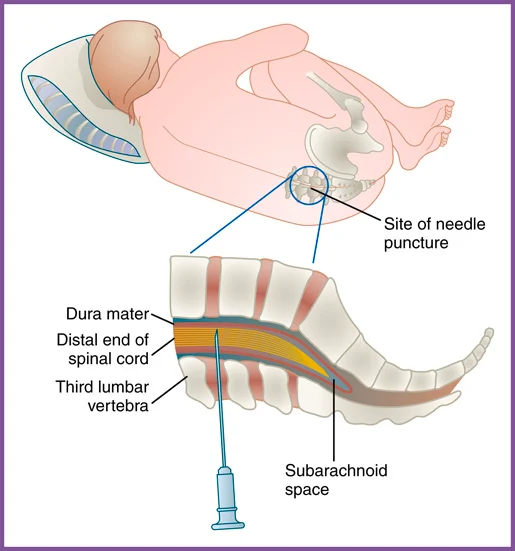
FIGURE 22.18 Lumbar puncture.
TABLE 22.5
Common Treatments Used for Nervous System Diseases and Disorders
| Normal CSF | Abnormal CSF and Related Conditions | |
|---|---|---|
| Pressure (mm H2O) | 70–180 | Increased: Increased intracranial pressure Decreased: Spinal cord tumor, fainting, diabetic coma, and shock |
| Appearance | Clear, colorless | Cloudy: Infection, elevated white blood cells or protein Bloody or red: Bleeding Brown, orange, or yellow: Increased protein or previous bleeding |
| Glucose (mg/dL) | 50–80 | Increased: Hyperglycemia (high blood glucose) Decreased: Hypoglycemia (low blood glucose), bacterial or fungal infection (e.g., bacterial meningitis), tuberculosis |
| Protein (mg/dL) | 15–60 | Increased: Blood in the CSF, diabetes, polyneuritis, injury, inflammation, infection, or tumor Decreased: Rapid CSF production |
| Blood Cells | 0–5 White blood cells (WBCs) 0 Red blood cells (RBCs) | Increase in WBCs: Meningitis, acute infection, tumor, abscess, stroke, multiple sclerosis Increase in RBCs: Traumatic lumbar puncture, bleeding into the CSF |
The medical assistant should coach the patient on the preparations for an EEG (see Procedure 22.4). In preparation for the procedure, patients should wash their hair the evening before or the morning of the procedure. They should not use any conditioner or hair care products (e.g., gels, hairspray). Using hair care products can interfere with the electrodes adhering to the scalp. Providers may have patients hold (not take) certain medications before the test if they may interfere with the EEG. Patients should avoid consuming any caffeine on the day of the test. If the EEG requires patients to sleep during the test, providers may encourage them to limit their sleep to 4 or 5 hours the night before.
Table 22.4
Common Treatments Used for Nervous System Diseases and Disorders
| Procedure | Description |
|---|---|
| Craniectomy | Surgical removal of a portion of the cranium. |
| Craniotomy | Surgical incision into the skull. |
| Neurectomy | Surgical removal of part or all of a nerve. |
| Neuroplasty | Surgery of the nerve. |
| Ventriculoperitoneal shunt | A catheter is inserted into the brain and drains extra fluid from the brain ventricles into the abdominal cavity. |
During the procedure, the patient will be relaxing in a bed or reclining chair. The technician will apply 16 to 25 electrodes to the scalp, either with a cap or paste. The wires from the electrodes bring the electrical impulses to the computer. The electrical activity in the brain is then recorded. The technician will record brain activity while the patient is at rest or asleep and with activities and stimuli (e.g., bright flashing light). The test takes between 45 minutes and 2 hours.
Once the test is done, the electrodes are removed, and the paste is removed with warm water. If the patient was given a sedative, no driving is allowed after the test. Mild skin irritation may occur for a few hours after the test. The patient should be informed of when to restart medications and when to anticipate the test results.
Assisting with Treatments
Learning Objective: Describe the medical assistant’s role in treatments for neurologic diseases.
Patients with neurologic diseases may be treated with surgical procedures (TABLE 22.5), or they may be prescribed a variety of medications. The following are some of the more common classifications of medications:
• Analgesic: Relieves pain.
• Anesthetic: Produces local anesthesia (no loss of consciousness).
• Anti-Alzheimer: Used to treat AD by increasing naturally occurring substances, such as acetylcholine, in the brain.
• Anticonvulsant: Reduces the frequency and severity of seizures by reducing excessive stimulation of the brain.
• Antidepressant: Used to treat depression, anxiety, and other neurologic disorders.
• Antimigraine: Alters circulation to the brain and is used to treat migraine headaches.
• Corticosteroid: Used to treat chronic inflammatory and some autoimmune diseases (e.g., multiple sclerosis).
Refer to TABLE 22.6 for information on the medication classification, including indication for use, desired effect, side effects, adverse reactions, and generic and trade names. Medical assistants should be familiar with medications that are prescribed to patients.